Article Text

Abstract
Background Aspirin inhibits colorectal carcinogenesis. In a randomised double-blind placebo-controlled trial, daily soluble aspirin significantly reduced recurrence of colorectal adenomas at 1-year follow-up. In this study the results of daily intake of low-dose aspirin on polyp recurrence at 4-year follow-up are presented.
Methods 272 patients (naive for chronic aspirin use) with colorectal adenomas were randomly assigned to treatment with lysine acetylsalicylate 160 mg/day (n=73) or 300 mg/day (n=67) or placebo (n=132) for 4 years. The primary endpoints were adenoma recurrence and adenomatous polyp burden at year 4, comparing aspirin at either dose with placebo. The same endpoints were also assessed at year 1 or 4 (last colonoscopy performed for each patient).
Results At the final year 4 colonoscopy the analysis included 185 patients (55 receiving aspirin 160 mg/day, 47 aspirin 300 mg/day and 83 placebo). There was no difference in the proportion of patients with at least one recurrent adenoma between patients receiving aspirin at either dose and those treated with placebo (42/102 (41%) vs 33/83 (40%); NS) or in the adenomatous polyp burden (3.1±5.8 mm vs 3.4±6.2 mm; NS). Also, the proportion of patients with at least one advanced recurrent adenoma did not differ (10/182 (10%) in the aspirin group vs 7/83 (7%) in the placebo group; NS).
Conclusion Daily low-dose aspirin decreased adenoma recurrence significantly at 1 year but not at year 4. This discrepancy might be explained by a differential effect of aspirin according to the natural history of the polyp.
Trial Registration Number NCT 00224679.
- Colorectal adenoma
- chemoprevention
- acetylsalicylic acid
- randomised controlled trial
- cancer prevention
- nutrition
- obesity
- cyclooxygenase-2
Statistics from Altmetric.com
- Colorectal adenoma
- chemoprevention
- acetylsalicylic acid
- randomised controlled trial
- cancer prevention
- nutrition
- obesity
- cyclooxygenase-2
Significance of this study
What is already known about this subject?
Long-term use of low-dose aspirin reduces the risk of colorectal cancer.
Aspirin also reduces the incidence of colon adenomas, especially when used for >10 years.
Controversy remains about the potential clinical value of low-dose aspirin and its consistency over time.
In spite of an unclear risk/benefit ratio, aspirin chemoprevention should still be implemented in high-risk patients with colorectal cancer.
What are the new findings?
The performance of three colonoscopies per patient (one at baseline with ablation of all polyps discovered, the second at 1 year and the third at 4 years) allows the distinction between an aspirin effect on missed polyps and on the occurrence of true new polyps.
Daily low-dose aspirin decreased adenoma recurrence significantly at 1 year but not at 4 years.
How might it impact on clinical practice in the foreseeable future?
These findings suggest a differential effect of aspirin according to the natural history of the polyp: a true chemopreventive effect observed only after 7–10 years which is distinct from the ‘anti-tumour’ effect observed at 1 year.
These results add new information which may be helpful for therapeutic decision-making.
Introduction
Cohort and case–control studies1–14 show that long-term low-dose aspirin reduces the risk for colorectal cancer (CRC), with risk reductions of 15–40% in meta-analyses.15 16 After a diagnosis of CRC, aspirin is associated with lower risks of disease-specific and overall mortality.17 It reduces the risk of colon adenomas and CRC, especially when used for more than 10 years,15 18 19 and it provides protection from experimental carcinogenesis.1 20 21
Seven randomised placebo-controlled clinical trials (RCTs) of aspirin for preventing CRCs or adenomas have been reported, four of which relate to CRC. The first trial found no effect of aspirin 325 mg every other day among healthy male physicians.22 23 The second trial found no effect of aspirin 100 mg every other day for 10 years in healthy US women.24 The other trials were primarily designed to assess the effects on vascular diseases.25 26 A recent meta-analysis of four randomised trials with 20-year follow-up showed that aspirin taken for several years at doses of at least 75 mg/day reduced CRC incidence and mortality.27 In three other trials adenomas were assessed. In the first trial, 325 mg/day aspirin was compared with placebo in 635 patients with a history of CRC. At interim analysis, aspirin significantly reduced the incidence of new adenomas by 35%.28 The second adenoma trial compared aspirin in doses of 81 mg/day and 325 mg/day with placebo in 1121 patients with a history of one or more colorectal adenomas and found a reduction in the risk of recurrence which was statistically significant only for the dose of 81 mg/day (RR 0.81; 95% CI 0.69 to 0.96).29 The third trial was performed in 945 patients with adenomas >5 mm in diameter removed during the 6 months before inclusion. After 3 years of follow-up, 99 of 434 patients (23%) receiving aspirin 300 mg/day had recurrence compared with 121 of 419 patients (29%) receiving placebo (RR 0.79; 95% CI 0.63 to 0.99).30
The clinical value of the preventive effect of aspirin on adenoma recurrence is controversial.31 32 Information is lacking on which subgroups would benefit most from aspirin, the optimum dose and the duration of treatment. The risk-to-benefit ratio of aspirin is hampered by its side effects. Indeed, evidence has accrued that treatment of many people to prevent a few CRCs is of questionable value, especially when even rare side effects can adversely affect the risk-to-benefit balance. In 1996 we planned a double-blind placebo-controlled RCT of soluble aspirin (160 or 300 mg/day lysine acetylsalicylate) on secondary prevention of colorectal adenomas after colonoscopic clearance of pre-existing polyps in a population at high-risk of recurrence. Only one follow-up colonoscopy was performed in previous studies, so the possible part of missed adenomas on the apparent effect of aspirin could not be assessed. By contrast, the design of our trial allowed distinction between new polyps and missed polyps. The 1-year results have been published previously.33 We present here the final 4-year results on adenoma recurrence and adenomatous polyp burden (APB).
Methods
Patients
The protocol of our multicentre trial performed in 51 French gastroenterology departments has been published previously.34 We included patients aged 18–75 years who had undergone a colonoscopy for which the bowel had been prepared adequately and the cecum visualised. Polyps were considered as proximal when located from the cecum to (but not including) the splenic flexure and as distal when located from the splenic flexure to the rectum. All polyps detected before randomisation were removed and measured. Polyps had to be removed within 3 months prior to inclusion in the study. All patients had a clean colon and rectum at study entry and after each following colonoscopy. Eligible patients were those judged able to follow the protocol who had either at least three adenomas irrespective of size or at least one measuring ≥6 mm in diameter, pathologically confirmed, with no history of CRC, familial adenomatous polyposis, bowel resection, life-threatening disease or an indication for chronic aspirin use. Patients were aspirin-naive at study entry and agreed not to use aspirin regularly all through the study (ie, for 7 consecutive days for at least 3 weeks per year or for >21 days throughout the year). Patients who successfully completed the 4-week run-in period by consuming at least 80% of the 300 mg daily dose of aspirin were randomly assigned in a three-group parallel design to either placebo or soluble aspirin in a dose of 160 mg/day or 300 mg/day. Figure 1 shows the flowchart of the trial.
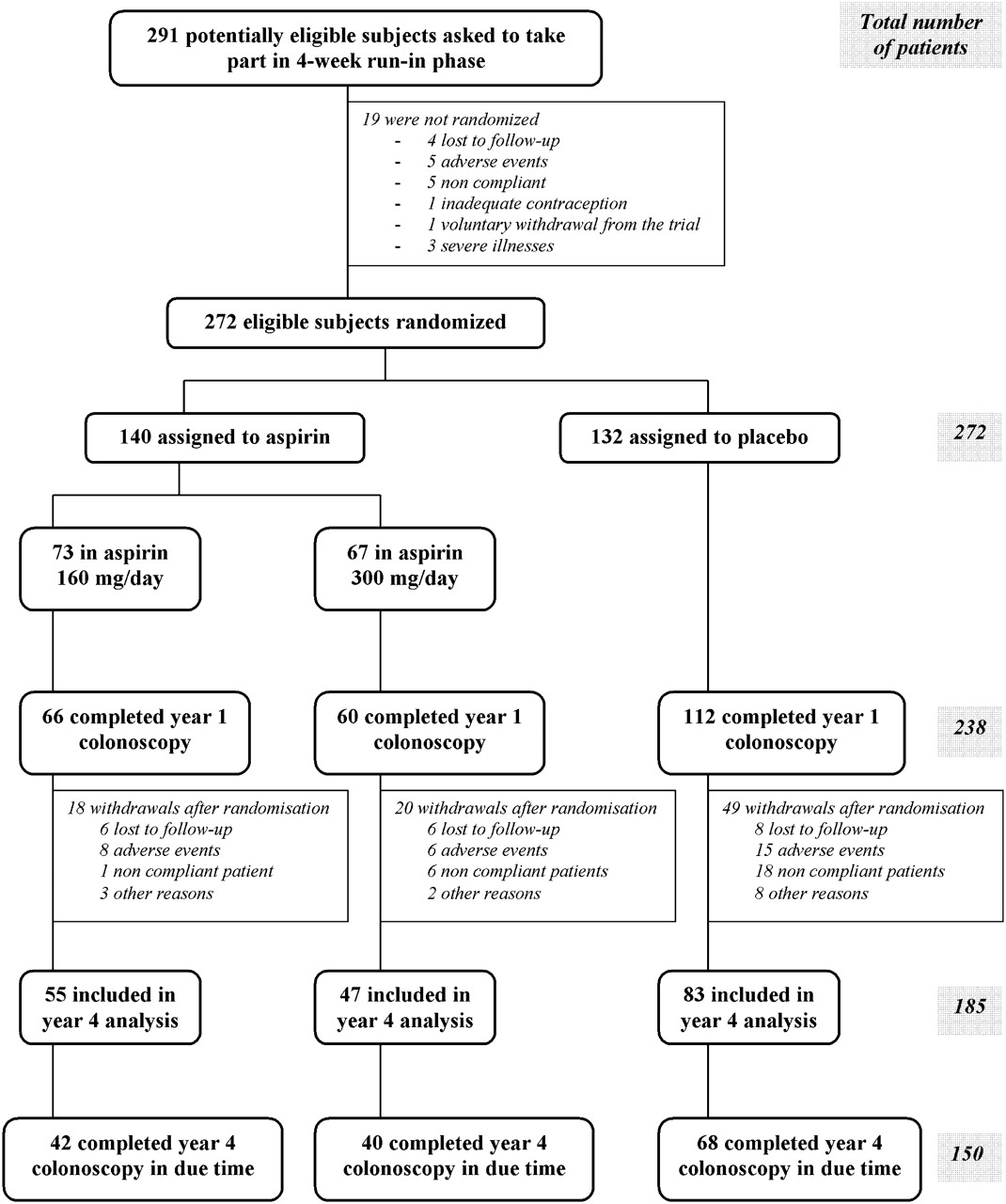
{kind=link}
Flow chart of the APACC trial. Year 4 analysis corresponded to all patients who completed year 4 colonoscopy, either in due time or not. Year 4 colonoscopy was considered to be in due time if it was performed from 6 months before to 6 months after the year 4 visit.
The primary outcomes were the proportions of recurrent adenomas and APB calculated as the sum of the diameters of these adenomas for each patient at the final colonoscopy at year 4. Ancillary outcomes were mean numbers of recurrent adenomas and numbers of recurrent advanced adenomas, defined as those with a maximum diameter of at least 10 mm, at least 25% villous elements or evidence of high-grade dysplasia. A secondary analysis was performed using the same parameters at the last colonoscopy for each patient 1 or 4 years after enrolment.
Study design
Randomisation, performed by the APACC Coordination Centre using a computer-assisted method, was balanced every four patients: one of each four patients received 160 mg aspirin, one 300 mg aspirin and two placebo (computerised randomised blocks). Lysine acetylsalicylate was administered in the form of one sachet to be diluted in a glass of water. Placebo was made of the same excipient as the active treatment and had the same appearance and taste. Patients, staff in the APACC Coordination Centre and study investigators were unaware of treatment assignment. Treatments, delivered in sequentially numbered containers prepared by a pharmacist prior to the beginning of the trial, were allocated by the independent Coordination Centre which was in charge of randomisation, preparation and distribution of treatment packages. Information about compliance and side effects was collected at regular visits every 4 months by senior gastroenterologists. Recruitment began in October 1996 and ended in February 2000. The trial was completed at the end of September 2005.
Statistical analysis
The statistical analysis was planned to assess first the effect of either dose of aspirin (160 mg/day or 300 mg/day) and placebo and, only in cases of a statistically significant overall effect of aspirin, to compare each dose separately with placebo. The primary endpoints were the effect of aspirin on the recurrence rate of one or more adenomas at the last follow-up colonoscopy (whether it occurred at 1 or 4 years) and the evolution of APB. We also analysed patients who experienced the 4-year colonoscopy either in due time (from 3 months before to 3 months after the 4-year visit) or not. All comparisons were performed by intention-to-treat analysis. Assuming an annual recurrence rate of adenomas of about 10% with a 4-year recurrence rate estimated at 43% and a drop-out rate of 15% over the 4-year period, this trial was initially designed to have at least 80% power to detect a reduction of 40% in recurrence rate using a two-sided test at the 5% significance level. With these assumptions, the recruitment target was 267 patients.
The results are presented as means±SD. χ2 tests were used to compare categorical variables and parametric tests for continuous variables which were approximated to normal law, an approach allowed by the large numbers of patients and the coherence between these tests and the multivariate analysis. In the multivariate analysis of the 4-year recurrence rate with multiple covariates (baseline characteristics), the magnitude of the treatment effect and of the recurrence rate was expressed as RR with 95% CI. p Values <0.05 were considered as statistically significant (two-tailed tests) and were adjusted for multiple testing. The analysis was performed using SAS software V.9.1.
Results
Patient characteristics
Of the 291 patients with adenomas confirmed by colonoscopy who entered the 4-week run-in period, 272 took at least 80% of the 300 mg daily lysine acetylsalicylate dispensed and thus were deemed eligible for the trial and randomised. Seventy-three patients were allocated to aspirin 160 mg/day, 67 to aspirin 300 mg/day and 132 to placebo. Baseline demographic and clinical characteristics of patients were similar among the aspirin and placebo groups at entry (table 1), except for a higher proportion of adenomas >10 mm among patients receiving aspirin. At baseline colonoscopy, only 13 of the 668 polyps excised from the 272 patients were lost (2%). Among the 655 excised polyps which underwent pathological examination, 549 were adenomatous and 85 were hyperplastic polyps.
Baseline characteristics of the intention-to-treat population of patients
Among the 272 randomised patients, 238 (87.5%) had a colonoscopy 1 year after enrolment (figure 1). At 4 years, 185 patients (68% of the initial population) had a third colonoscopy, 150 in due time according to the protocol (within 3 months before or after the foreseen time of 4 years after inclusion) and 35 not in due time: 55 were taking aspirin 160 mg/day, 47 aspirin 300 mg/day and 83 placebo. This imbalance was mainly due to non-compliance (see figure 1). Of the 150 patients (55% of the initial population) who had a 4-year colonoscopy in due time and did not present any major protocol violation, 42 were receiving aspirin 160 mg/day, 40 aspirin 300 mg/day and 68 placebo. During the whole trial, 122 patients had at least one major protocol violation: 32 in the group receiving aspirin 160 mg/day, 27 in the group receiving aspirin 300 mg/day and 63 in the placebo group (NS). Among the 87 patients who did not complete the year 4 colonoscopy, 29 withdrew from the trial for adverse events, 25 for non-compliance, 13 for other reasons and 20 were lost to follow-up. More patients dropped out after randomisation in the placebo group than in the aspirin group (49/132 (37%) vs 38/140 (27%); χ2 =3.1; p=0.08), possibly due to a higher rate of non-compliance in the placebo group (18/49 (37%) vs 7/38 (18%); χ2=1.9; p=0.17). Among those who completed the year 4 colonoscopy, compliance with the study treatment during the 4-year follow-up, assessed by counting returned sachets, was high (mean±SD 88±26%) and similar between the groups.
Results at 4 years (main analysis)
Among the 185 patients who had a third colonoscopy at 4 years, 15 of 55 who received aspirin 160 mg/day (27%) had at least one recurrent adenoma compared with 27 of 47 (58%) who received aspirin 300 mg/day and 33 of 83 (40%) patients in the placebo group (NS; table 2). Mean±SD APB was not statistically different between aspirin at either dose and placebo (3.1±5.8 mm for aspirin and 3.4±6.2 mm for placebo; NS). Concerning the ancillary end-points, the mean±SD number of recurrent adenomas was significantly lower in patients who were treated with aspirin 160 mg/day than in those in the placebo group (0.4±0.7 vs 0.8±1.3, p=0.025). The proportion of patients with at least one recurrent advanced adenoma was similar in the three groups (table 2). Table 3 shows the distribution of patients with or without at least one recurrent adenoma at year 1 and year 4 in both treatment groups.
Main final results of primary endpoints using two modes of analysis
Distribution of the patients with or without at least one recurrent adenoma at year 1 and at year 4 in aspirin and placebo groups
Results at last follow-up (1 or 4 years)
At last follow-up colonoscopy, 244 patients who underwent either 1-year or 4-year colonoscopy were available for analysis: 32 of 68 patients (47%) who had received aspirin 160 mg/day had at least one recurrent adenoma compared with 33 of 60 patients (55%) who had received aspirin 300 mg/day and 62 of 116 (54%) given placebo (RR for both doses of aspirin combined 0.95; 95% CI 0.75 to 1.21; NS). Mean±SD APB was 6.3±11.4 mm among the 116 patients given placebo and 4.1±6.7 mm among the 128 patients treated with either dose of aspirin (p=0.06). The mean±SD number of recurrent adenomas per patient, an ancillary endpoint, was 1.5±2.4 in the placebo group and 1.0±1.5 among those in the two aspirin groups (p=0.07, table 2). Additionally, aspirin at either dose did not decrease the proportion of patients with at least one adenoma >5 mm or 10 mm. The proportion of patients with at least one recurrent advanced adenoma was not statistically different with aspirin at either dose or with placebo (14% and 16%, respectively). Analyses adjusted on initial APB or number of polyps showed similar results.
Multivariate analysis showed that final recurrence was more frequent among men than women (RR 0.67; 95% CI 0.42 to 1.04; p=0.06) and among patients aged ≥65 years than among younger patients (RR 1.44; 95% CI 1.00 to 2.07; p=0.07). Final recurrence was statistically more frequent in patients with a personal history of adenoma before inclusion (RR 1.58; 95% CI 1.13 to 2.22; p=0.01), in patients with an initial polyp burden >10 mm (RR 1.45; 95% CI 0.97 to 2.17; p=0.06), in those taking aspirin at either dose with at least three adenomas at initial colonoscopy (RR 2.10; 95% CI 1.22 to 3.61; p=0.01) and in patients taking aspirin with at least two adenomas at 1-year colonoscopy (RR 2.67; 95% CI 1.37 to 5.21; p=0.004).
Adverse events
A few serious adverse events occurred during the trial. There was one unrelated death and one myocardial infarction in the placebo group and one stroke in the aspirin group. No major bleeding occurred in either the aspirin and placebo groups. Twenty-four patients receiving aspirin had a minor bleeding episode compared with 20 receiving placebo. Twenty-nine patients withdrew from the trial for adverse events after randomisation (8 receiving aspirin 160 mg/day, 6 aspirin 300 mg/day and 15 placebo).
Discussion
This RCT compared two doses of lysine acetylsalicylate (160 mg/day or 300 mg/day) with placebo. The 4-year final results in 185 patients of the 272 initially randomised did not show a preventive effect of aspirin on adenoma recurrence or APB. Adenoma recurrence at year 4 was predicted by a personal history of adenoma before inclusion, at least three adenomas at inclusion and by 1-year recurrence. These findings contrast with the preventive effect at 1 year: 68 of 112 patients (59%) in the placebo group had at least one recurrence compared with 59 of 126 (46%) receiving either dose of aspirin (p=0.04). Aspirin significantly decreased APB at 1 year. At the last follow-up colonoscopy (year 1 or 4), adenoma recurrence and APB showed a borderline statistical significance in favour of aspirin.
The discrepancy between our results at 1 and 4 years could have two explanations. An obvious reason could be the lack of statistical power of the final analysis because of the number of drop-outs (32%). Between the 1-year and 4-year analyses there were 53 drop-outs, mainly due to the long duration of follow-up and the need for a third colonoscopy. An alternative reason for the discrepancy could be a differential effect of aspirin according to time of exposure and to the natural history of the polyps. Our design allowed distinction between the effect of aspirin on missed polyps and new polyps. The discrepancy might be related to a less marked and less immediate effect of aspirin on true new polyps, as previously suggested.35 36 The putative true antiproliferation effect of relatively high doses of aspirin (300 mg/day) might explain the preventive effect at 1 year. The absence of effect at 4 years would indicate that this genuine chemoprevention might be observed at low doses only after longer periods of treatment (10 years), as previously shown.10 14 15 27 The borderline preventive effect observed at the final colonoscopy (1 or 4 years) is in keeping with other studies that found no distinction between the 1-year and 3-year results.29 30
Another limitation of this study was the non-significant imbalance between the numbers of patients receiving aspirin and placebo from year 1 to year 4. There were more withdrawals in the placebo group (mainly for non-cooperation), a finding attributable to a progressive and partial loss of blinding related to the absence of minor bleeding, leading some patients to guess that they were not taking aspirin. The concomitant use of potential chemopreventive agents such as other non-steroidal anti-inflammatory drugs (NSAIDs), glucocorticosteroids, calcium or vitamin D appeared to have a limited influence (if any) on the results.
Our study did not allow a precise comparison between the two doses of aspirin. Only two conflicting animal studies have assessed the preventive effect of two doses of aspirin on polyp recurrence.37 38 The doses used in these studies (10–30 mg/kg) were much higher than in humans (2–4 mg/kg).
Table 4 shows the main results of the four RCTs of secondary prevention of adenoma recurrence by aspirin. Our study is characterised by a higher risk of recurrences, more than 50% in the placebo group compared with 29% in the study by Logan et al30 and 27% in the study by Sandler et al.28 Only Baron et al29 had a similarly high risk of recurrence (47%). Some discrepancies between trials could be explained by these differences in levels of risk for adenoma. Despite a higher recurrence rate, the overall exposure to aspirin expressed in patient-years was lower in our study because fewer patients were included (table 4). A meta-analysis of 3000 patients from the four RCTs found a significant decrease of 17% in adenomas and a 28% reduction in advanced lesions.38 The greatest benefit of aspirin appeared during the first year of treatment.39 Contrasting with the trials of Baron et al29 and Logan et al,30 we did not find any chemoprevention by aspirin of recurrence of advanced adenomas, a rare event. In a recent RCT in Lynch syndrome, aspirin (600 mg/day) had no effect on colon adenomas or carcinomas and on APB compared with placebo.40
Effects of aspirin on adenoma recurrence compared with placebo in the four published randomised controlled trials
Aspirin inhibits cyclooxygenase-2 (COX-2). Other NSAIDs (sulindac, cyclo-oxygenase-2 inhibitors) also decrease colorectal adenomas.41–50 Since CRCs51–64 and colorectal adenomas65–76 often overexpress COX-2, as we have also shown,77 aspirin probably acts by inhibiting COX-2. Aspirin only reduced the risk of those CRCs overexpressing COX-2.78 However, NSAIDs decrease proliferation and increase apoptosis of CRC cell lines without COX–2 activity.79–81
In conclusion, aspirin did not reduce adenoma recurrence or APB at year 4 follow-up, in contrast with its beneficial effect at 1 year. This should be considered when planning an interventional study. However, low-dose aspirin might be used in secondary chemoprevention in addition to colonoscopy39 82 in high-risk patients. These patients, because of their age and comorbidities, may also have an increased risk of cardiovascular disease. The prediction of high-risk patients most likely to benefit from aspirin and the best dose and minimum duration of treatment are issues that remain to be resolved.13 14 27
Acknowledgments
The authors thank the patients who participated in the study, P E Douziech for coordination of treatments and the hospital pharmacists for preparation of the treatments in the trial centres, and Mrs C Coutinho for her help in typing the manuscript.
Appendix
APACC Study Group
The APACC group included all physicians who were involved in the project at all stages.
Participating gastroenterologists:
Attar A; Barakrok N; Beaujard E; Bejou B; Benamouzig R; Benazzouz AP; Benoit R; Berthelemy B; Blondon H; Bordet E; Boulant J; Bour B; Cassan P; Chaussade S; Ciribilli J-M; Coudert P; Couturier D, Courillon-Mallet A; Danielou J-Y; Degoy J; Delasalle P; Delchier J-C; Dieumegard B; Dreyfus G; Dupas J-L; Durney D; Dusoleil A; Flamenbaum M; Flaubert G; Fontanges T; Fourgeaud J-L; Gatineau-Saillant G; Godeberge P; Goldfain D; Gouffier E; Grobost O; Heyman B; Heyries L; Humeau B; Kalinsky E; Kerneis J; Klewansky M; Kusielewicz D; Lagneau M; Lamarque D; Lepage M; Loiseau D; Macaigne O; Malka D; Marill J-L; Marti R; Mitry E; Nalet B; Nizou C; Pariente E A; Paupard T; Perrot S; Pigot F; Pouderoux P; Rampal P; Rautureau J; Renou C; Ribiere O; Roche H; Rotenberg A; Rougier P; Ruszniewski P; Schneider S; Souillac P; Stremsdoerfer N; Tainturier M-H; Travers B; Vergeau B; Zamora C; Zummer K.
Participating pathologists:
Abarah B; Aillet G; Anger E; Balaton A; Barhoum K; Baron V; Benderitter-Giovo E; Bertrand G; Besnard-Bernadac M-C; Bonnafous F; Bouc M; Bougaran J; Bringeon B; Cales V; Calvet E; Carayon M-J; Carnot F; Chamlian A; Chassaigne C; Chatelain D; Chomarat C; Cloup N; Coppe P; Costes-Chalret N; Cousin-Maignan C; Degott C; Dubois-Gordeff A; Durand L; Fabiani-Caetz B; Forest E; Giglio L; de Pinieux G; Gros P; Hofman-Guilaine C; Homsi T; Jeandel R; Journel B; Kalifat R; Karkouche B; Kerlo P; Lab P; Languille-Mimoune O; Lesec G; Longchampt E; Louis B; Marquet M; Martin A; Marty-Double C; Medioni L-D; Molas G; Monnier P; Mosnier-Damet M; Nenert N; Petit J; Rey C; Richard-Coulet E; Rolachon J; Romeo J-M; Roucayrol A-M; Roux F; Saint-Paul M-C; Schill H; Schlund-Schoettel E; Staroz S; Trincard M-D; Tulliez M; Valade S; Verdier V; Verriele V; Zafrani E.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Download Supplementary Data (PDF) - Manuscript file of format pdf
Footnotes
↵* The APACC study group participants are listed in Appendix 1.
Funding This trial was supported by grants from the French Ministry of Health (PHRC) and AP-HP, from the Association pour la Recherche contre le Cancer (ARC), the Société Nationale Française de Gastroentérologie (SNFGE). A special non-restricted grant was provided by Sanofi-Synthelabo. This trial was supported by public research funds. Lysine acetylsalicylate (Kardegic) and placebo were kindly supplied by Sanofi-Synthelabo. None of the authors or collaborators had any financial relationship with Sanofi-Synthelabo. Funding sources did not interfere at all with trial design, data collection, analysis and interpretation, neither with the writing of the present article nor with the decision to submit it for publication.
Competing interests None.
Patient consent Obtained.
Ethics approval The study protocol was approved by the ethics committee of Saint-Germain-en-Laye Hospital, France.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Data and pathological collection is available for scientific sharing.
Linked Articles
- PostScript