

Abstract
Comprehensive and spatially mapped molecular atlases of organs at a cellular level are a critical resource to gain insights into pathogenic mechanisms and therapies tailored to the disease of each patient. Obtaining rigorous and reproducible results from disparate methods and at different sites to interrogate biomolecules at a single cell level or in 3-dimensional (3D) space is a significant challenge that can be a futile exercise if not well controlled. The Kidney Precision Medicine Project (KPMP) is an endeavor to generate 3D molecular atlases of healthy and diseased kidney biopsies using multiple state-of-the-art OMICS and imaging technologies across several institutions. We describe a pipeline for generating a reliable and authentic single cell/region 3D molecular atlas of human adult kidney with emphasis on quality assurance, quality control, validation and harmonization across different OMICS and imaging methods. Our “follow the tissue” approach encompasses sample procurement to data generation, analysis, data sharing, while standardizing, and harmonizing procedures at sample collection, processing, storage and shipping. We provide key features of preanalytical parameters, bioassays, post analyses, reference standards and data depositions. A pilot experiment from a common source tissue processed and analyzed at different institutions was executed to identify potential sources of variation, feasibility of multimodal analyses and unique and redundant features of the macromolecules being characterized by each technology. An important outcome was identification of limitations and strengths of the different technologies, and how composite information can be leveraged for clinical application. A peer review system was established to critically review quality control measures and the reproducibility of data generated by each technology before granting approval to work on clinical biopsy specimens. This unique pipeline establishes a process that economizes the use of valuable biopsy tissue for multi-OMICS and imaging analysis with stringent quality control to ensure rigor and reproducibility of results and which can serve as a model for similar personalized medicine projects.
Author Contributions MTE, RM, BBL, TS, TA, AS, SP, CRA, DD, EAO, SW, GZ, MJ and KD performed the ground work for the quality control group, wrote the KPMP TIS manual of procedures and generated figures. HH, JZ, RS, RM, TS, EAO, MTE, TME, PH, SP, MK, ZL and SJ generated the initial working reference marker list. CEA, TME, JBH, JL, MK and SJ led the Pilot 1 protocol. TME, VD, LB, JG, CEA, ZL, SJ and JBH developed the pathology QC tissue qualification and tissue processing criteria. JBH organized and executed the Pilot tissue collection and distribution. JC designed the SpecTrack system. CP prepared and organized the TIS manual of procedures and performed data organization services. YH led ontology development for QC metadata and knowledge standardization. BS and EA organized data integration efforts and data authentication in the data hub. KS and MS led the OMICS discussion group. SJ led the quality control group. TME and CEA led the tissue processing group. MTE and SJ led the Molecular and Pathology Integration group. MTE and SJ conceived and led the TISAC process. RI, OGT KZ, ZL, PH, BR, PCD, KS, MS, JBH, CEA, LB, JG, TME, MK and SJ conceived the integrated TIS pipeline and QC vision. TME and SJ wrote the initial draft of the paper. All authors contributed to the writing and editing of the manuscript.
Introduction
Recent advances in biotechnology allow capturing the state of a tissue in health and disease at an unprecedented structural and molecular resolution (1). Application of these technologies at the level of the genome, transcriptome, proteome and metabolome have enabled identification of regulatory cascades and their mapping into tissue compartments at a single cell resolution (2–8). There is a unique opportunity in applying these technologies to clinical samples to decipher the complexity of tissue architecture when evaluating intrinsic organ function and its dysregulation in disease.
Kidney diseases are well-poised to be evaluated by a tissue driven approach as nephrologists routinely use kidney biopsies in a clinical setting for diagnosis and management. Using bulk and tissue compartment microdissection, first insights have been obtained by integrating histology, morphometry, transcriptional profiles and clinical outcomes primarily in glomerular diseases (9). While these studies identified therapeutic targets and disease endophenotypes, they were limited to the evaluation of glomerular diseases in routine biopsies and the analysis of tissue compartments consisting of a multitude of interacting cell types (9). Recognizing this opportunity, National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) initiated the Kidney Precision Medicine Project (KPMP) with the explicit goal to bring the biomedical advances of tissue level disease process mapping to the two most devastating renal diseases, chronic kidney disease (CKD) and acute kidney injury (AKI), with a prevalence as high as 14% (37 million people) for CKD (10). In a sequential process, KPMP is establishing a framework to ethically and safely obtain research kidney biopsies from study participants with CKD and AKI, using a sophisticated tissue acquisition protocol specifically tailored to enable downstream emerging molecular genome scale analyses at tissue and cell level resolution. As KPMP sets out to establish a lasting resource both for tissue and tissue derived omics data sets, rigorous pre-analytical and analytical protocols with highly standardized and controlled workflows are considered an essential prerequisite for the success of the project. Here we describe a quality-controlled tissue interrogation pipeline established in the KPMP for multimodal analysis of kidney biopsies using various omics and imaging technologies. Our pipeline realizes the power of combined analyses of well vetted and curated data from different technologies to ensure rigor, reproducibility and complementarity to generate molecular atlases of healthy and disease kidneys that can impact patient care, while extracting maximum data from a limited amount of tissue. The framework established serves as a paradigm for similar atlas efforts and precision medicine projects of other organs systems and diseases (1, 3, 11, 12).
Approach
Overview of KPMP technologies: creating a molecular and functional kidney map
The KPMP encompasses a diverse set of technologies to generate a robust molecular, spatial and structural atlas (Fig.1, 2). A multimodal interrogation of various biomolecules including RNA and protein purposely enables a comprehensive coverage and identifies unique as well as non-captured (“blind spots”) features of each technology. Redundancy among the different technologies further provides orthogonal validation that lends confidence to the discovered genes/proteins/metabolites/cell types and cell states. The overall vision enables the interrogation of the same tissue from the same study participant using many different technologies by harmonizing processing and preservation steps, to enhance data quality and to identify weaknesses and strengths of each applied technology (Fig. 2 and see later). Following is a brief overview of technologies in the KPMP to generate a biomolecular/cell atlas of the human healthy and diseased kidney.

IU-Indiana University; OSU – Ohio State University; UCSD – University of California, San Diego; WU – Washington University in St. Louis; UM – University of Michigan; UCSF – University of California, San Francisco; UTHSA – University of Texas Health Sciences, San Antonio; PNNL – Pacific Northwest National Laboratory; EMBL – European Molecular Biology Laboratory.
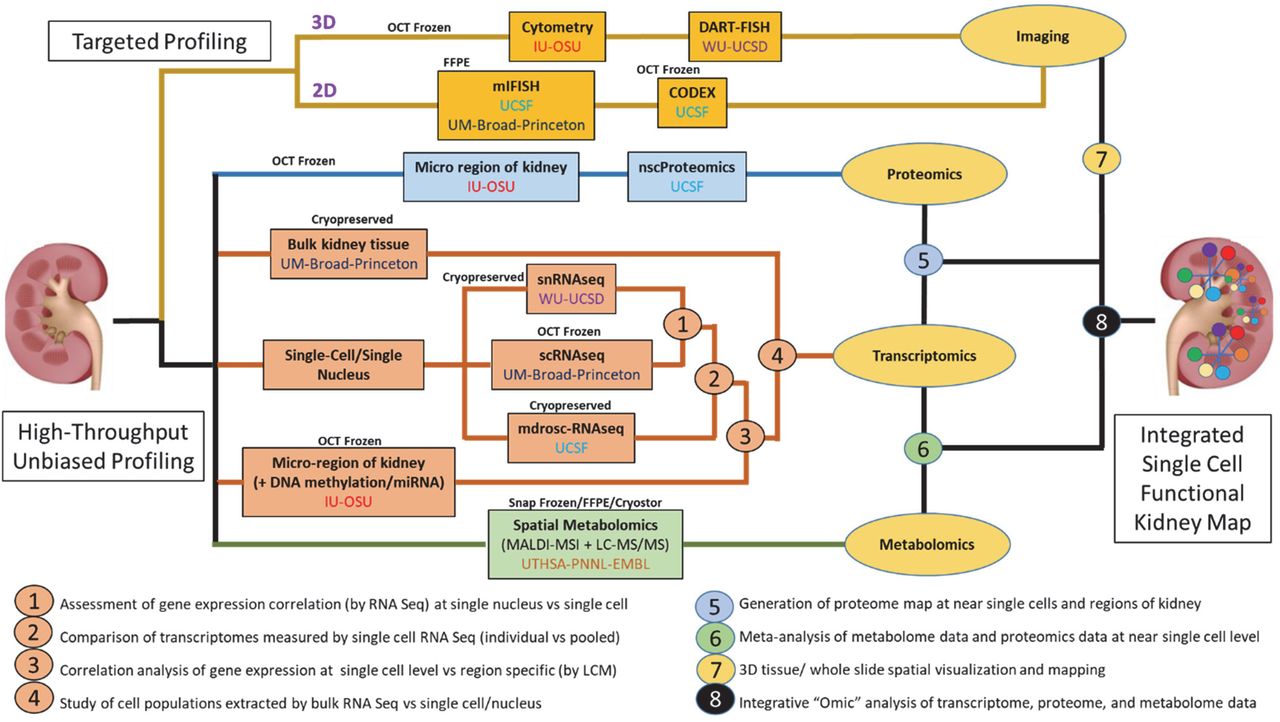
Envisioned pathway template of detailed tasks and steps of the processes leading to the kidney atlas.
Transcriptomics
Several technologies are generating gene expression data at bulk, regional and single cell level for comprehensive coverage of the transcriptome for the reference (relatively healthy or pathologically normal) and disease atlases (AKI and CKD subtypes). Single nucleus (sn) (UCSD/WU) and single cell (sc) (UCSF and Premiere-Michigan/Broad/Princeton sites) RNA-seq technologies are being used for cataloging molecularly-defined cell populations for the generation a single cell kidney atlas (13–15). Each of these technologies uses different approaches in sample preparation, dissociation or processing that have unique advantages and disadvantages (see TIS protocol on https://kpmp.org/researcher-resources/). Given the potential to introduce artifacts or miss cell types due to processing of these specimens, concurrent bulk RNA expression analysis on undissociated tissue or regional laser microdissection (LMD) (IU/OSU) is performed (16–18). Using the LMD technology, transcriptomic signatures are identified for seven sub-segments of the nephron including the proximal tubule (PT), thick ascending loop of Henle (TAL), distal convoluted tubule (DCT), collecting duct (CD), as well as compartment-specific signatures for glomeruli, the tubulo-interstitium (TI), the interstitium (without glomeruli or tubules), as well as a bulk cross-section of the entire biopsy. LMD transcriptomic signatures can serve as an important independent validation measure that provides regional spatial context to cell populations discovered using single cell technologies. To complement the mRNA signatures obtained from the single event technologies and regional transcriptomics, miRNA sequencing of bulk cross-sections from the same OCT-embedded core are sequenced specifically for small RNA (IU/OSU) (19).
Proteomics
Two different approaches were planned in the KPMP to generate reference and diseased kidney proteome. The regional/segmental approach by the IU/OSU group combines the collection of specific regions of the kidney using LMD with quantitative proteome analysis using state-of-the-art HPLC/mass spectrometry (MS) instrumentation to generate agnostic global profiles of the glomerular and tubulo-interstitial compartments with high sensitivity and reproducibility (20). The UCSF group is employing recently developed nanoscale proteomics analysis in which a few cells can be processed to generate cell-specific protein profiles (21). Combining this technology with regions isolated by LMD provides regional and spatial definitions of generated proteome data. Both technologies additionally provide bulk proteomics data on tissue sections allowing cross platform/site analysis.
Metabolomics
The UTHSA/PNNL group will generate spatial metabolomics measurements by using matrix-assisted laser desorption/ionization (MALDI) mass spectrometry imaging (MSI), an approach that has been utilized previously for kidney molecular imaging (22, 23). Here, fresh-frozen tissues are cryosectioned, mounted on optically transparent and electrically conductive slides, coated with an organic matrix that assists in facilitating desorption and ionization of endogenous molecules, and serially probed with a laser to attain mass spectral information at predefined locations. They employ two different platforms to generate metabolite profiles that are designed for cross validation and complementarity. An important aspect is that data are processed using the METASPACE platform (24, 25) (a tool developed by the EMBL portion of this group), which is an automated molecular annotation engine that enables data visualization and co-registration with other optical images.
2D and 3D Imaging
There are several imaging technologies within KPMP that inform on precise 2D and 3D expression relationships of biomolecules, cells and structures with varying degree of multiplexing, spatial resolution and tissue preservation conditions (Fig. 2). The UCSD/WU group will develop DART-FISH to delineate single cell mRNA expression of several hundred transcripts in each cell at high resolution in 3D using high resolution confocal microscopy. The UCSF and PREMIERE sites will use miFISH to generate simultaneous gene and protein expression data at the single cell level in 2D space (26). The IU/OSU site will utilize large scale 3D confocal imaging of longitudinal kidney thick sections probing concurrently for 8 different targets using antibodies or fluorescent small molecules, followed by tissue cytometry analysis (27, 28). Prior to any staining, this technology uses label-free imaging to determine tissue integrity using endogenous fluorescence and quantify collagen deposition using second harmonic generation. The resulting image volumes undergo cytometry analysis with a customized Volumetric Tissue Cytometry and Analysis (VTEA) software. This approach allows the interactive exploration of the image volumes, as well as quantitative analysis of the abundance, distribution, and other 3D spatial features of interest for various cell types, based on supervised and unsupervised analytical approaches (29). The UCSF site will use Co-detection by indexing (CODEX) (30), an orthogonal approach to perform 2D profiling in situ on up to 30 antigens at single-cell resolution on a single tissue section using antibodies labeled with unique oligonucleotide tags (“barcodes”). The labeling and detection is done in an iterative manner in groups of two or three targets per cycle by fluorescent dyes labeled with oligonucleotide sequences (“reporters”) corresponding to a given subset of antibody barcodes; in each cycle the previous reporters are removed and a new set is introduced. The montage image consisting of all signals from each cycle is analyzed for marker intensity distribution across the tissue section, for cell count of a given cell population defined by marker sets and for spatial relationship between cell populations of interest in the specimen (30).
Guiding principles for multimodal quality-controlled tissue interrogation
Biomolecular and imaging data to build a kidney atlas in KPMP consists of partnerships between multiple institutions as Tissue Interrogation Sites (TISs) to generate various single cell/region OMICS (transcriptomics, proteomics and metabolomics) and 2D and 3D high resolution kidney imaging data using technologies described above (Fig. 1, 2). These multi-scalar imaging and single cell/region omics technologies provide an unprecedented resolution, big data for interpretation and insights into biological processes. With these attributes comes the challenge of compounding errors as the data are dependent on multiple processes and steps that begin from specimen procurement to data generation and analysis. When data are generated from different institutions and on archived tissues there are several other sources of random and technical variations that confound the outcomes and impact biological reproducibility and interpretation of data. An additional challenge is maximizing the application of these sensitive, big data technologies to clinical biopsies with limited tissue available for research. Motivated to overcome these challenges in KPMP, our approach described here aims to standardize and harmonize, where possible, the entire process of tissue procurement all the way up to analysis. Key factors considered were economizing tissue usage, maximizing preservation and use for multiple technologies, and documenting quality of intermediate steps with clearly defined quality assurance and control criteria. Central to this theme was the application of rigorous procedures for transparency, technical and biological reproducibility across multiple sources of tissue procurement, analysis and interpretation. Below we provide an overview of the approach, examples of different technologies including current quality control metrics, procedures for harmonization and standards to be met for interrogating human kidney biopsies.
Overview of the strategy: “Follow the tissue”
An overall goal of our approach is to derive synergistic and integrated information on the biological state of tissue in health and disease. Anticipating that the tissue would come from different sites, our approach was to develop a tissue processing pipeline that can be easily implemented at the bedside and applied to multiple state-of-the-art interrogation technologies. We required that each technology independently investigates and analyzes adult human kidney tissue in a reproducible and rigorous manner. The goal for this approach was to demonstrate feasibility, perform validations, harmonize procedures and enable integrated analysis with other technologies executed in KPMP (Fig. 2). This process posed several challenges at multiple steps in the “follow the tissue” process including variable standards in collecting metadata, procurement, processing, sample preparation, analytical parameters, analysis and data sharing and deposition. To tackle these challenges, we formed working groups for tissue processing that included expertise in OMICS, imaging, and pathology. These groups addressed quality control measures across four main categories: 1) Participants, 2) Tissue, 3) Assays and analysis, 4) Data hub (Fig. 3). Each category encompassed various components with parameters for quality assessment and control. The working groups met weekly through web-conferences and offline with concrete action items and delegated tasks to identify critical parameters and data to be collected in each of the 4 categories. These meetings were open to all KPMP members and meeting minutes were documented at the KPMP management website in “Basecamp” (www.basecamp.com). This process enabled easy access to archived documents and meetings, and active discussions among members. A critical aspect was formulating and capturing well-vetted relevant metadata in each of these categories to enable the interpretation of molecular discoveries among the underlying biological variations related to healthy and disease phenotypes (Table 1). We established benchmarks for the entire process, and a clear approach for data visualization and sharing for various types of users. Once the overall vision or “blueprint” was established, the pipeline was pressure-tested with a pilot project using adult human kidney tissue (see later). We describe below the individual steps of this workflow.

Subject Metadata
Detailed relevant participant associated metadata including demographics, clinical and pathological diagnoses, comorbidities, medications, social histories and laboratory data were identified through a team effort of all the recruitment sites and TISs and will be described elsewhere. This was important to interpret variations in data due to contributions of patient attributes. For example, sex differences, age, race or medications such as diuretics or antihypertensives can contribute to changes in molecular or cellular distribution of transporters in the kidney. An example of the main standardized patient metadata fields used by all the sites is provided (Table 1). These metadata fields are being modeled and represented using the Kidney Tissue Atlas Ontology (KTAO)(31), and Ontology of Precision Medicine and Investigation (OPMI) (32), two open source biomedical ontologies that are being developed by the collaborative KPMP and ontology communities.
Tissue Preanalytical Considerations
The output of OMICS and imaging technology results is intimately related to tissue handling and preservation attributes, which if not controlled can contribute to technical variations and decreased data quality. Since there are more than 10 tissue interrogation technologies but only sparse tissue availability (biopsy), the methods in which tissue is collected, preserved, processed, stored, shipped, analyzed and recorded were harmonized, whenever possible, to minimize technical variations (some discussed below). Several preanalytical parameters for quality control related to specimen handling, processing, preservation, orientation, quantity used, shipping and storage were identified to minimize these concerns (Table 1). An infrastructure to track specimen movement from origin to specimen processing sites was developed (SpecTrack). A key feature was the ability to record deidentified specimens and documentation of the time and state in which the specimens are shipped and received accompanied with a photograph of the contents. All the sites were required to show successful use of this system prior to being qualified to receive specimens. An important consideration in designing the pipeline was to assess the quality and composition of the tissue being analyzed to best interpret the molecular outcomes. While some technologies depended on complete dissociation of tissue (scRNA-seq) others had the opportunity to register tissue composition before dissociation or analysis. As such, guidelines were developed by the KPMP pathologists and TIS investigators for high level quality assessment of composition and integrity of tissue sections and included relative proportions of cortex, medulla, glomerulosclerosis and features compromising integrity such as necrosis and hemorrhage (Table 1).
Tissue Analytical and Assay Considerations
There were three main tenets we focused on: 1) Assay metadata, 2) Assay quality assurance (QA) parameters, and 3) Assay quality control (QC) parameters. We ensured careful attention was made from the beginning to define and record all the metadata associated with the assays, with the goal of transparency and reproducibility. QA is linked to understanding and applying the best practices recommended in the field for that particular technology, using a specific instrument set(s), protocols or platform. The reliance on data from the manufacturer or post-marketing analysis when available is essential. We ensured that all platforms used in data production are optimized to produce the best possible results or operating under bone fide core facilities. For the QC component, we expected to meet and exceed a set of criteria guaranteeing that the assay works properly; these criteria also set a benchmark to give reproducible data for building the kidney atlas.
Considering the complexity of assays and data outputs across technologies, our goal was to harmonize metadata collections, assays, instrumentations and post hoc analyses for similar biomolecules where possible. During sample preparation for assays and analysis, quality control parameters and minimum attributes that are relevant for the performance of the assay were identified and common terms were used for similar types of technologies (RNA or protein or imaging). Key parameters needed to be identified for each technology to be captured during assays that could be tracked to monitor quality at different time points throughout the respective pipeline. Each technology was expected to come up with concrete criteria for quality control measures and to demonstrate pass-fail rates and reproducibility in pilot experiments (see later). Furthermore, within each technology, implementation of measures that allow detection and control of batch effects and assay drift were also incorporated.
We followed the concept of building an iterative marker list derived from published data and data generated from the KPMP to qualify the identity and composition of the tissue being interrogated, validate and optimize tissue processing pipelines and identify regions or cell types for integrative quality check and analysis to build the kidney atlas. Our initial list (made in 2018) of a subset of cell type markers mainly relied on rodent studies and bulk RNAseq data with corresponding evidence from the human protein atlas (Supplemental File 1) (33–42). Later iterations of the potential cell types/states were heavily dependent on the data generated from the human kidney specimens derived in part from the pilot project (see below). Similarly, for imaging studies a number of parameters were established to best standardize the formats of image acquisition, analysis and deposition (Supplemental Table 1).
Data quality check, visualization and sharing
We placed additional quality checks for the generated data by establishing a non TIS directed team in “data hub” where the investigators could seamlessly transfer data upon passing their QC checks. Among the functions of the “data hub” are: 1) the examination of the associated metadata for completeness, 2) independent analysis of the data for passing quality control thresholds, 3) enhancing data availability to other KPMP sites for integrated analysis and quality check and 4) planning for public sharing. Indeed, an essential component of data output is making it accessible to the public. In this regard, the KPMP data hub is tasked with a team dedicated for building tools for summary analysis and visualization of the integrated results generated by the various technologies.
Anticipated challenges and how to handle them: harmonization vs complementarity, and the need for a pilot experiment
Based on the overall vision of the “follow the tissue” pipeline, many challenges were anticipated because of the extensive breadth of the technologies applied to interrogate common specimens. How do we reconcile outputs from these various approaches? Is it possible to store and ship tissue to distant sites without compromising it for interrogation by different technologies? How do we benchmark the quality control parameters for evolving technologies, while at the same time economizing and maximizing the use of precious tissue? Within each technology, can we define steps in the analytical pipeline that could be harmonized with other technologies without undermining the uniqueness and value presented by each technology alone? Can we strike the appropriate balance between harmonization and complementarity? Indeed, such balance would solidify the overall approach and potentially become a strength and a staple of KPMP to promote discovery. To tackle these challenges and demonstrate the feasibility of the analytical pipeline, we recognized that the “follow the tissue “approach required testing in a consortium wide experiment. Therefore, a KPMP pilot experiment was designed and executed as described below.
Testing the quality control pipeline: a consortium wide pilot experiment
Rationale
The objective of this experiment was to use a same source kidney specimen to pressure-test our “follow the tissue” approach on a consortium level. We aimed to assess our ability to 1) standardize tissue processing/handling, storage and shipping steps; 2) establish feasibility and validate the Q/A-Q/C parameters for all the technologies in the interrogation pipeline; 3) compare, when applicable across sites, the performance of molecular interrogation and identify sources of variabilities and concordance; 4) lay out a blueprint for harmonization and complementarity across technologies; 5) identify gaps and weaknesses in the interrogation pipeline. An important outcome was to define a protocol that is harmonized across technologies, and that could ultimately be used for interrogating biopsies from patients. This protocol is also expected to economize the use of limited tissue material for diagnostics and research.
Design
The approach for the pilot was to collect tumor-free kidney cortex from nephrectomy specimens from the University of Michigan tissue collection center, preserve the tissue in different types of media according to the needs of the various TISs and distribute to each TIS for testing feasibility, validation and identifying the quality control metrics for their respective technologies. Contiguous serial sections (approximately 1cm x 2mm x 2mm) in the shape of rectangular cuboids were cut for processing and preservation (FFPE, fresh frozen OCT, flash frozen in liquid nitrogen, Cryostor, RNAlater) and shipped to each TIS designated by a code (Figure 4 and Supplemental Figure 1). In total, 6 different nephrectomy specimens were processed as described above and used by all the TISs. Hence, not only each site had access to the same tissue source, but there were also 6 biological replicates distributed for the purpose of testing reproducibility, as discussed below.
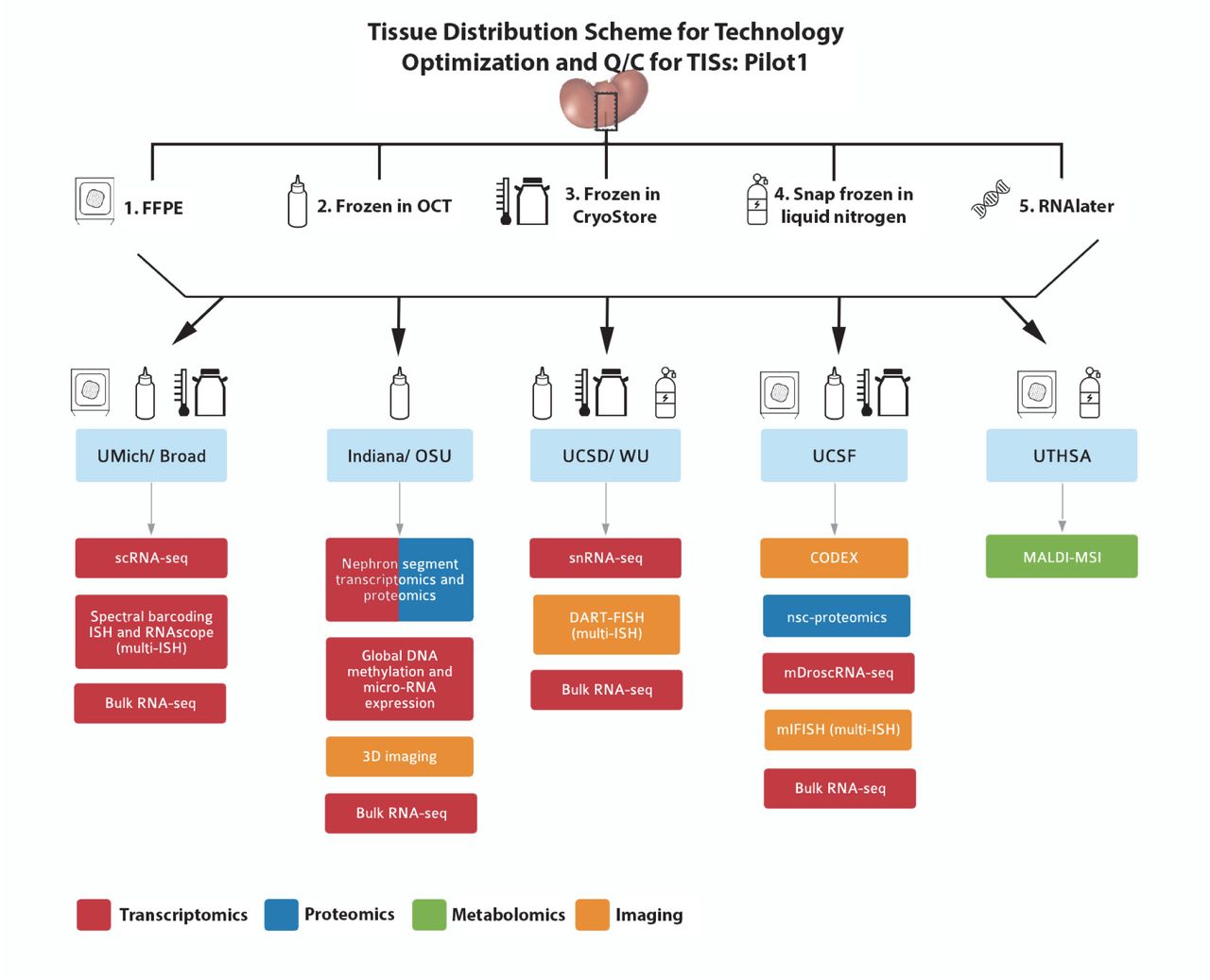
A single source kidney tissue from a tumor nephrectomy was sectioned into equal blocks (schema in supplemental figure 1) and processed into 5 tissue processing methods according to the downstream applications listed. Blocks of the tissue was distributed to the sites according to the technology as indicated by the drawings. Formalin fixed paraffin embedded (FFPE); in-situ hybridization (ISH); single cell (sc) and single nuclear (sn) RNA sequencing (RNA-seq). Near single cell (nsc)-proteomics; matrix-assisted laser desorption/ionization mass spectrometry imaging (MALDI MSI).
Quality control outcomes and observations based on the pilot experiment
Tissue procurement/preservation - Preanalytical parameters: The following outcomes were directly derived from this pilot experience:
Better definition of the metadata associated with tissue procurement, preservation, integrity and composition. We identified commonalities between tissue procurement, processing, assessment and storage that enabled the use of similar conditions for multiple technologies (Table 1). For example, snRNAseq, 3D-mass cytometry, LMD transcriptomics, LMD proteomics, mDroscRNAseq, spatial metabolomics, miFISH and DART-FISH could all use fresh frozen OCT blocks (Tables 2, 3 and detailed in TIS manual of operations at www.kpmp.org/resources).
Ontology-based metadata modeling and representation. Such an approach will likely facilitate the definition of the metadata and make the links between different metadata types more meaningful and machine-interpretable, supporting advanced data analytics and knowledge discovery.
Real time testing of specimen tracking using the SpecTrack software. This live tracking of the tissue revealed weaknesses in the pipeline and allowed improvements, including better documentation of tissue and temperature states of shipments and appropriate packaging materials (Supplemental Figure 2).
Effect of shipping and best practices establishment. To determine the effect of shipping on tissue quality, an assessment of RNA integrity was performed on bulk tissue preserved in RNAlater using independent RNA preparation methods at two different sites. All the bulk RNA samples (total 12, 6 nephrectomy samples in RNAlater shipped to each site) were sequenced at a central site. These results showed strong correlation among adjacent tissue samples from the same subject for all 6 subjects and established the shipping conditions that do not adversely affect tissue state as measured by RNA expression and integrity analysis (Figure 5).
Initial processing at the TISs. This experiment also provided an opportunity to examine the initial processing steps at each TIS, to explore the potential of standardizing common procedures, whenever possible. This resulted in the implementation of common procedures at each site, which were incorporated in the KPMP TIS manual of procedures (www.KPMP.org). For example, this pilot experiment identified the need to obtain histology sections flanking areas of interrogation within the tissue, to inform on the state, composition, and orientation of the tissue. This process also allowed the same OCT block to be exchanged by two interrogation sites to perform successful molecular interrogation simultaneously with 3 different techniques (Figure 5). The pilot experiment was also crucial to verify, validate and expand the metadata variables that needed to be captured for faithful documentation of the tissue journey from harvesting to interrogation.
Analytical Q/C parameters for each technology based on pilot 1: One of the main goals of this experiment was to test and validate the quality control parameters for each technology in each site. This experiment also presented a venue to test for both biological and technical reproducibility. There were in total 6 different nephrectomy specimens distributed to each site, with a substantial amount of tissue from each specimen. As such the TISs were able to optimize their technologies, check feasibility and in parallel apply the refined methods to their locally collected kidney samples. Repeat testing on a single specimen provides a framework for technical reproducibility; the use of tissue from different donors and tissue from different sources (pilot and local samples) ensured testing the methodologies for rigor and biological reproducibility. The Q/C parameters adopted by each technology based on this pilot experiment are summarized in Tables 2, 3 and 4.
Solidification of Q/C parameters was also performed by cross-validation with existing data/standards or by cross-validating outcomes from various technologies performed on the single source kidney tissue provided in this pilot. This cross-validation could be in the form of concordant readouts, such as detection of the same molecules/metabolites in the same samples using different technologies. In addition, orthogonal validation could also occur using concordant “derived” readouts such as pathway analyses. For example, the TIS technologies can detect different genes/molecules/metabolites, but these molecular entities can be part of the same signaling pathway. Examples of orthogonal validation approaches are shown in Figure 5 and will be presented in detail in a separate manuscript.
Post-analytical outcomes: In addition to the cross-validation benefits discussed above, examining the outputs from various technologies promoted integration efforts and helped determine the extent of complementary information provided by each technology. This ensures that a comprehensive cellular and molecular converge is provided by the consortium to make robust kidney atlas and provide a platform for discovery.
This post-analytical exercise also provided the opportunity for further metadata harmonization, at the various levels of tissue processing, analytics and analysis. Additionally, parameters for diagnostic features, composition, and integrity of the tissue that are applicable to all the TISs were further refined and led to a protocol for interrogating patient biopsies in the KPMP described in a comprehensive Pathology protocol document (https://kpmp.org/researcher-resources/).
An additional important outcome was that significant amount of gene and protein expression data were generated from the pilot samples. These data collected from multiple sites provide an initial view of cellular diversity in the human kidney (Figure 6, Table 5). The analysis also revealed stress states related to processing of tissue and underlying pathology that could not have been predicted from gross evaluations in presumably healthy tissue. In fact, some novel discoveries have already emerged in the initial version of the kidney atlas from the Pilot project (13).
“*” denotes technologies approved by TISAC for interrogating patient biopsies (Oct 2019).
“*” denotes technologies approved by TISAC for interrogating patient biopsies (Oct 2019).
Asterisk denotes genes detected by more than one technology. Italics, genes detected by a single technology.

A) High correlation of bulk RNA seq from adjacent samples shipped and processed at different sites. B) Adjacent samples from same patient shipped to different TISs show different types of information from different technologies in KPMP with histological tissue composition verification for snRNAseq at WU-UCSD and label-free second harmonic generation highlighting extent of fibrosis at IU-OSU. C) Correlation between cell types and regions among snRNA-seq, LMD transcriptomics of the indicated regions by IU/OSU and between snRNA-seq and scRNA-seq. D) Economizing tissue usage by rotating fresh OCT frozen kidney tissue between IU and WU/UCSD. Here frozen sections were processed and analyzed for 3D tissue cytometry and LMD-RNA analysis and then the block was shipped to WU/UCSD for histological registration and subsequently generating snRNA-seq. Genes specific to each LMD compartment were determined by their upregulation in that compartment compared to other compartments as well as differential expression at a nominal p < 0.001. The UMAP plot shows the sample (~900 nuclei) contributing to many of the cortical cell types in the kidney snRNAseq atlas (~18000 nuclei) (13).

The nephron illustration is based on Kriz, W. & Bankir, L. A standard nomenclature for structures of the kidney. The Renal Commission of the International Union of Physiological Sciences(IUPS). Kidney Int.33,1–7 (1988). T, T lymphocyte; B, B lymphocyte; NK, natural killer cell; MAC, macrophage.
Identification of gaps and improvement of the process
An area of priority identified during the integration efforts of the large OMICS and imaging datasets was the need to establish benchmarks for the nomenclature of cell types, regions and associated genes, proteins and metabolites for reference and disease atlas and various injury states. A promising methodology of analysis that could link multiple technologies is a cell-centric approach, whereby the outputs can reflect changes at the cell level in a tissue specimen. This was essential as several groups are investigating the single cell transcriptome or proteome of the kidney but there is lack of conformity regarding nomenclature and annotations. However, this analytical process requires an initial definition of cell types based on a set of criteria, such as: gene expression (RNA and protein), cell state (baseline, stress, injury), spatial localization and associations, among others. The pilot studies generated an initial working list delineating the complexity of cell types and a subset of associated marker genes in the adult human kidney which could serve as a starting point for kidney OMICS and imaging studies for classification of cell types and states and harmonization with recent renal tubule epithelial cell nomenclature (Table 5) (42). An ontological representation of the cell markers has been initiated to seamlessly link gene, cell type and spatial tissue location at an integrative semantic level (31).
After establishing qualification criteria for tissue processing and the analytical process, a key question was if the technologies are ready to interrogate the limited clinical biopsy specimens. Therefore, it was unanimously perceived that a mechanism needs to be established to firmly vet and anchor each technology for quality control, rigor and reproducibility before handling any prospective precious biopsy tissue. This resulted in the establishment of a peer review technology approval process, which will be discussed below.
Implementation of best practices to perform tissue interrogation on KPMP biopsies: the TISAC process
Approval of TISs to receive biopsies for interrogation
To rigorously evaluate each technology and eliminate self-approved bias by each TIS we established a Tissue Interrogation Site Approval Committee (TISAC). This committee evaluates all technologies prior to approval to perform studies on KPMP biopsy samples. The committee is composed of representatives from the central hub, DVC, recruitment sites, other TISs, and external ad hoc members as required to provide sufficient expertise to review the technology. The committee organizes webinars for the TISs to receive feedback regarding technology readiness. A portfolio is submitted by a TIS for each technology which addresses the protocol, quality control metrics, sample handling, batch effects, assay drift and complementarity. These elements are summarized in Figure 7 and Supplemental file 2 [TIASC checklist]. Three primary reviewers formulate critiques after reviewing the portfolio, consult among each other and then the entire portfolio is discussed in a TISAC review call with representation from the TISs (except the TIS under review), non-TIS members and the NIDDK. The TISAC provides constructive feedback to enhance the reproducibility and complementarity of each technology, as well as identify areas that require additional supporting data. Once satisfied with a given technology’s readiness, the TISAC recommends approval and notifies the Steering Committee. The TISAC provides their report to the NIDDK and the KPMP external expert panel who ultimately approve the technology and TIS for receipt of patient samples. Each TIS is further expected to report on the state of their technology at least annually and sooner if there are any modifications in the protocol used.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
This workflow includes completion of a recorded webinar and submission of a portfolio that details the quality control metrics and technology outcomes. The TISAC reviews this material, providing recommendations to the tissue interrogation site for improvement before a site is approved to receive biopsies. The TISAC ultimately forwards their recommendations to the NIDDK and external expert panel (EEP) for final approval.
Ongoing progress, challenges and future outlook
Designing and implementing a quality control pipeline for the various technologies in KPMP required an a priori conceptualization of the scope, type and usefulness of the data that led to the “follow the tissue” pipeline concept with quality control components embedded throughout presented here. In addition to the expertise of investigators within and outside KPMP, we were also guided by the interaction with large national and international consortia. The validated pipeline that began as a concept provides a paradigm for similar efforts in healthy and disease atlas projects. The vision of KPMP is to evolve dynamically by incorporating ongoing progress in science, technology and patient care. Therefore, an important component of KPMP is an ability to identify opportunities to improve the quality control process, tackle challenges that are presented when changes are introduced by evolving or newer technologies, and mitigate potential threats or unforeseen errors. Examples of ongoing areas of development or topics that could present a challenge in the immediate future are described below:
Ontology representation of metadata types, cell markers, assays, and assay components to support harmonization. The urgency of this task has been recognized and has been the focus of dedicated workshops. In addition to linking the data, ontologies will be essential to link all the quality control elements within the data and metadata. The KPMP QC and ontology working groups are collaborating and making progress in “ontologizing” and linking different data types, cell markers, assays and assay components. KPMP is expected to define new landscape related to kidney disease specific ontologies that will be the subject of a separate publication.
DVC integration and dissemination of results. This area is currently in development. It is expected that data (raw and processed), metadata and all Q/C elements will be publicly available for all types of users in a way that is easy to query, access and interpret.
Incorporation of external data. The ability of the interrogation pipeline with its various technologies and Q/C elements to interact with external data will be important to extend the relevance and reach of KPMP discoveries.
Future proofing and addressing technology drifts.
A few of the key major future challenges are outlined in Table 6.
Conclusions
With the implementation of a multimodal and integrated pipeline for molecular interrogation of kidney biopsy specimens, the KPMP experience will be unique in its goals to set high standards for quality control, rigor and reproducibility. Vetted technologies participating in KPMP will undergo careful scrutiny to comply with these goals of quality control, while at the same time allowing a dynamic and iterative approach that promote improvement and transparency. In doing so, KPMP could become a model for other national and international efforts that also seek to decipher human disease and build a dynamic tissue atlas. KPMP’s ultimate goal is to improve patient care and cure kidney disease.
Acknowledgements
The Kidney Precision Medicine Project is supported by the National Institute of Diabetes and Digestive and Kidney Diseases through the following grants: UH3 DK114923, UH3 DK114920, UH3 DK114933, UH3 DK114937, UH3 DK114907, U2C DK114886. We thank the KPMP patient participants, Recruitment sites, Central Hub and all the TISs for many valuable discussions and feedback towards the QC efforts. We are grateful to the KPMP Publications and Presentation committee for suggestions and review of this manuscript. A complete list of all KPMP members can be found at kpmp.org.
Footnotes
REFERENCES




