

Abstract
Human skin contains a significant number of T cells that support tissue homeostasis and provide protective immunity. T cell function in human skin is difficult to study due to a lack of adequate in vivo models. In this study we used immunodeficient NOD-scid IL2rγnull (NSG) mice that carried in vivo-generated engineered skin (ES) and received adoptively transferred human peripheral blood mononuclear cells. ES were generated from keratinocytes and fibroblasts only and initially contained no skin-resident immune cells. This reductionist system allowed us to study T cell recruitment and function in non-inflamed and non-infected human skin. We found that functional human T cells specifically infiltrated the human skin tissue and responded to microbial antigen in vivo. Importantly, T cell maintenance and function was supported by the microenvironment of human skin. We have thus generated a novel mouse model with broad utility in studies of human cutaneous antigen-specific T cell responses and the role of the skin microenvironment to skin immunity in vivo.
Introduction
As the body’s outermost barrier, the skin represents a unique and complex immunological organ. As such, healthy human skin contains around twice the number of T cells found in the blood of which the majority are memory T cells (Bos et al. 1989; Clark et al. 2006) that support tissue homeostasis and ensure adequate response to pathogens (Di Meglio et al. 2011; Klicznik et al. 2018; Nestle et al. 2009). Although significant advances in understanding the role of the skin microenvironment on T cell function and memory development in murine skin have been made (Mackay et al. 2015; Mackay et al. 2013; Pan et al. 2017), the specific contribution of keratinocyte- and fibroblast-derived signals to cutaneous immunity in human skin remain poorly understood. T cell responses are strongly influenced by the surrounding tissue (Hu and Pasare 2013; McCully et al. 2012), and T cells at different barrier sites show distinct functional and metabolic properties (Kumar et al. 2017; Pan et al. 2017), therefore it is crucial to study cutaneous immunity within its physiological compartment in vivo. Due to fundamental structural differences between human and murine skin, as well as a lack of direct correspondence between human and murine immune cell populations (Di Meglio et al. 2011; Gudjonsson et al. 2007; Perlman 2016; Shay et al. 2013), direct translation from the murine cutaneous immune system can be difficult. This emphasizes the need for mouse models that faithfully replicate conditions found in human skin. Humanized mice, in which immunodeficient mice are adoptively transferred with human peripheral blood mononuclear cells (PBMC) and transplanted with human full thickness skin derived from either healthy donors or patients with skin diseases are currently used to study human skin immunology in vivo (Boyman et al. 2004; King et al. 2009; Watanabe et al. 2015). In these models the rejection of skin allografts and xenogenic graft versus host disease (GvHD) development can be readily studied (Racki et al. 2010), but antigen-specific activation of T cells has been much harder to follow. Additionally, if obtained from adult donors full-thickness skin grafts contain resident immune cells (Clark et al. 2006; Racki et al. 2010; Sanchez Rodriguez et al. 2014; Watanabe et al. 2015), making it difficult to functionally analyze and manipulate discrete skin-tropic T cell populations.
We hypothesized that humanized mice reconstituted with simplified human skin consisting only of keratinocytes and fibroblasts would provide a reductionist system allowing us to study human T cell recruitment and function in human skin in absence of acute inflammation. To this end, we used NOD-scid IL2rγnull (NSG) mice that were adoptively transferred with human PBMC and carried in vivo-generated engineered skin (ES). This model serves as a novel platform for studying human cutaneous antigen-specific T cell responses, and the contribution of the skin microenvironment to skin immunity in vivo. Additionally, we provide a method to stimulate robust antigen-specific memory responses of cutaneous T cells in this system.
Results
Human T cells specifically infiltrate human engineered skin in a xenograft mouse model
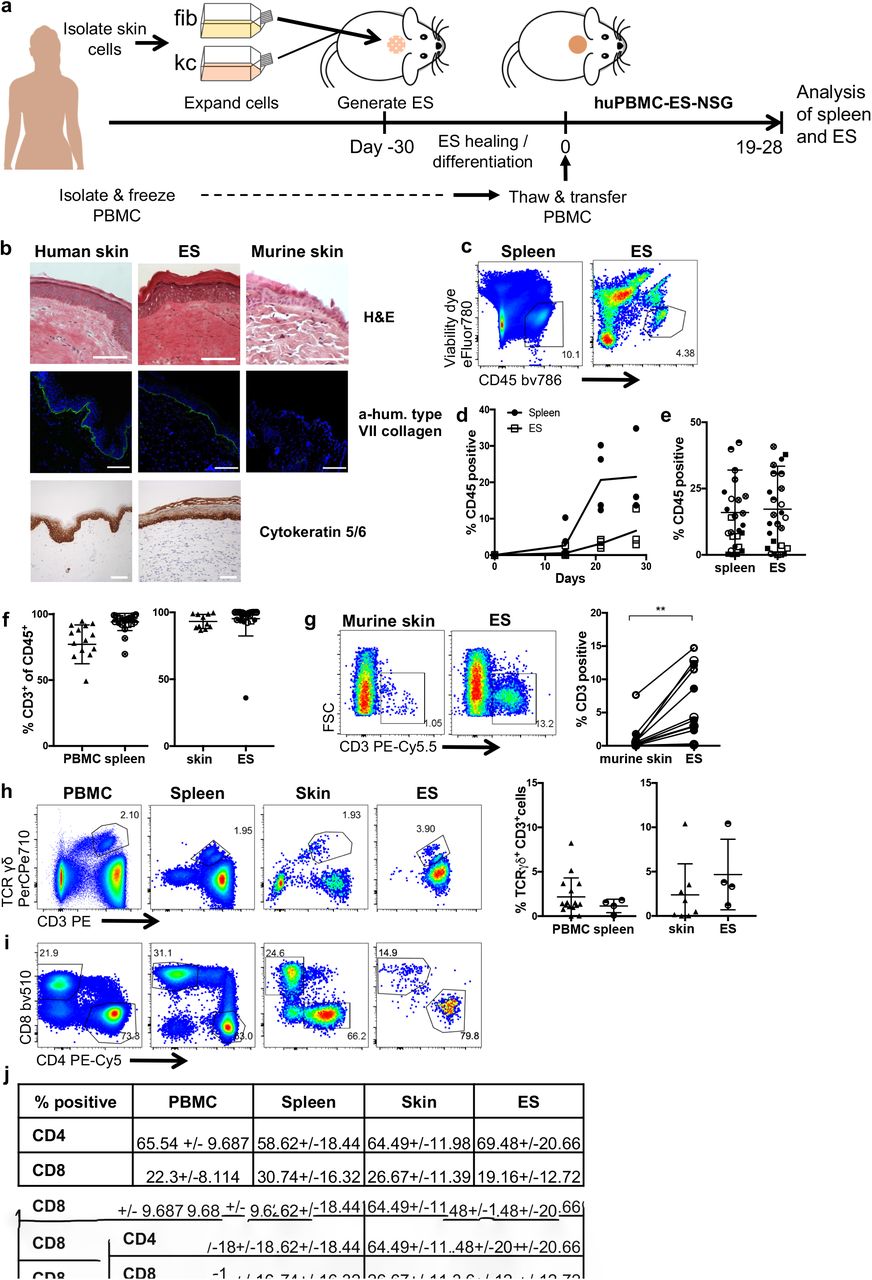
To follow human skin infiltration by autologous human immune cells, we generated engineered skin (ES) from human keratinocytes and fibroblasts isolated from healthy human skin and immortalized (Merkley et al. 2009). ES was generated as described before (Wang et al. 2000) and allowed to heal and differentiate for a minimum of 30 days (Fig.1a). H&E staining revealed that the ES displayed histological features of human and not murine skin. Additionally, organotypic proteins such as human type VII collagen at the basement membrane of the ES and human cytokeratin 5/6 within the correct epidermal layers of the ES confirmed correct differentiation and human origin (Fig.1b). In parallel, human PBMC from the skin donor were isolated and stored in liquid nitrogen until use (Fig.1a). After complete wound healing of the ES PBMC were adoptively transferred, thus creating a mouse model designated huPBMC-ES-NSG.
Engraftment of human CD45+ cells was detectable after 14 days in the spleen and after 21 days in the ES (Fig. 1c-d). After a period of 18 – 34 days mean levels of human CD45+ cells in spleen and ES were at >18% (Fig. 1e). The majority of human cells (>94%) in spleen and ES were CD3+ T cells (Fig. 1f) and human CD3+ cells preferentially infiltrated human ES not the adjacent murine skin (Fig. 1g). CD4+ and CD8+ as well as TCRγδ+ T cells engrafted within the spleen and ES at levels comparable to human PBMC and skin (Fig. 1h-i). The ratios of CD4+ and CD8+ T cells engrafting in spleen and ES reflected the physiological levels found in human PBMC and skin, respectively (Table in Fig. 1j).

(a) Schematic of the huPBMC-ES-NSG model. (b) H&E staining and immunofluorescence staining of human type VII collagen in human skin, ES and murine skin, as indicated (upper two panels) as well as immunohistochemical staining of human Cytokeratin 5/6 in human skin and ES (lower panel). White bar = 100µm (c-g) Single cell suspensions of spleen and ES of huPBMC-ES-NSG mice were analyzed by flow cytometry. Each data point represents an individual human donor or experimental mouse. Circles represent data collected from huPBMC-ES-NSG mice using tissue of donor WT85 and squares donor WT70. The different fillings of the symbols indicate independent experiments. (c) Representative flow cytometry analysis and (d) graphical summary of proportion of human CD45+ cell as % of live cells in the lymphocyte gate in spleen and ES at indicated time points after adoptive transfer of 2.5×106 PBMC. (e) Graphical summary of proportion of CD45+ cells of live cells in spleen and ES 18-34 days after PBMC transfer. n=3-6/experiment; cumulative data of 5 independent experiments. (f) Graphical summary of the proportion of CD3+ cells of live CD45+ cells (g) Representative flow cytometry analysis and graphical summary of CD3+ percentages in ES and adjacent murine skin gated on live lymphocytes. n=3-6/experiment; cumulative data of 3 independent experiments. Significance determined by paired student’s t test; mean +/- SD. (h) Representative plots and graphical summary of γδ+ and CD3+ cells of live CD45+ in indicated tissues. (i) Representative flow cytometry plots of CD4+ and CD8+ of CD3+CD45+ live gated cells (j) Summary of CD4 and CD8 expressing cells in human PBMC and skin and spleen and ES, gated on live CD3+CD45+ lymphocytes. n=3-6/experiment; Combined data of 6 independent experiments.
In previous studies development of xenogeneic graft versus host disease (xeno-GvHD) occurred around 5 weeks after adoptive transfer of 107 human PBMC into NSG mice (Ali et al. 2012; King et al. 2008). To delay the development of GvHD we reduced cell numbers to 1.8 - 3×106 /mouse. Additionally, we limited all experiments to 35 days, which was before onset of GvHD thus avoiding convoluting effects on our studies.
Taken together, these data illustrate that the human T cell compartment can be reconstituted in spleen and ES of the huPBMC-ES-NSG mouse. Next, we sought to determine whether the model was suitable to study human T cell function within human skin in vivo.
Cutaneous and splenic T cells from huPBMC-ES-NSG maintain the functional profile of T cells found in human skin and blood
We assessed the function of splenic and skin T cells following ex vivo stimulation and intracellular cytokine staining. Production of the Th2, Th17 and Th22 cytokines IL-13, IL-17 and IL-22, respectively, were preserved in CD4+ T cells isolated from the huPBMC-ES-NSG mouse when compared to T cells from human blood and skin(Fig. 2a-b; e-g). By contrast, increased percentages of CD4+ T cells isolated from the spleen and ES produced GM-CSF (Fig. 2c; h-i). Interestingly while IFNγ+CD4+ cells were increased in the spleen when compared to PBMC, the proportion of IFNγ producing CD4+ cells within the ES was comparable to skin from healthy donors (Fig. 2i). In addition to conventional T cells, CD4+CD25+Foxp3+ regulatory T cells engrafted within the spleen and ES (Fig. 2d; j). Analogous to the cytokine profiles of splenic and cutaneous CD4+ T cells, we assessed the cytokine secretion of CD8+ T cells isolated from spleen and ES (Fig. 3). The cytokine profiles of CD8+ T cells in ES and spleen were comparable to healthy human skin and PBMC with the exception of GM-CSF, which was increased within the ES, similar to the CD4+ T cell population.

(a-c) Single cell suspensions of blood and skin of healthy donors and spleen and ES of huPBMC-ES-NSG mice were stimulated ex vivo with PMA/ionomycin and intracellular cytokine production was analyzed by flow cytometry. Representative analysis of IL17, IL22, IL13, GM-CSF and IFNγ % of CD4+ cells as indicated and (d) CD25 and Foxp3 expression by gated CD4+CD3+CD45+ live leukocytes. (e-j) Graphical summary of the expression of the indicated markers by T cells from blood and skin of healthy donors and spleen and ES of huPBMC-ES-NSG mice by gated CD4+CD3+CD45+ live leukocytes. n=3-6/experiment; cumulative data of 2-5 independent experiments as indicated by the symbol fillings.

(a-e) Graphical summary of flow cytometry analysis of IL17, IL22, IL13, GM-CSF and IFNγ producing CD8+CD3+CD45+ gated live leukocytes from blood and skin of healthy donors and spleen and ES of huPBMC-ES-NSG mice as indicated upon ex vivo stimulation with PMA/Ionomycin and intracellular staining. n=3-6/ experiment; combined data of independent 1-4 experiments.
Engrafted T cells share a skin-homing memory-like phenotype
Since CD4+ T cells represent the majority of skin-homing and -resident T cells (Clark et al. 2006; Watanabe et al. 2015), we focused on the function of cutaneous CD4+ T cells. Confirming previous studies of PBMC engraftment in NSG mice, we found that human CD4+ T cells isolated from mice did not express markers of naïve T cells such as CCR7 and CD45RA despite being present in the ingoing PBMC population (Ali et al. 2012) (Fig. 4a). Additionally, around half of them expressed cutaneous leukocyte antigen (CLA), a glycan moiety that promotes skin-homing (Clark et al. 2006) (Fig. 4b). Taken together these data indicate that engrafted CD4+ T cells show a skin-tropic, memory-like phenotype.
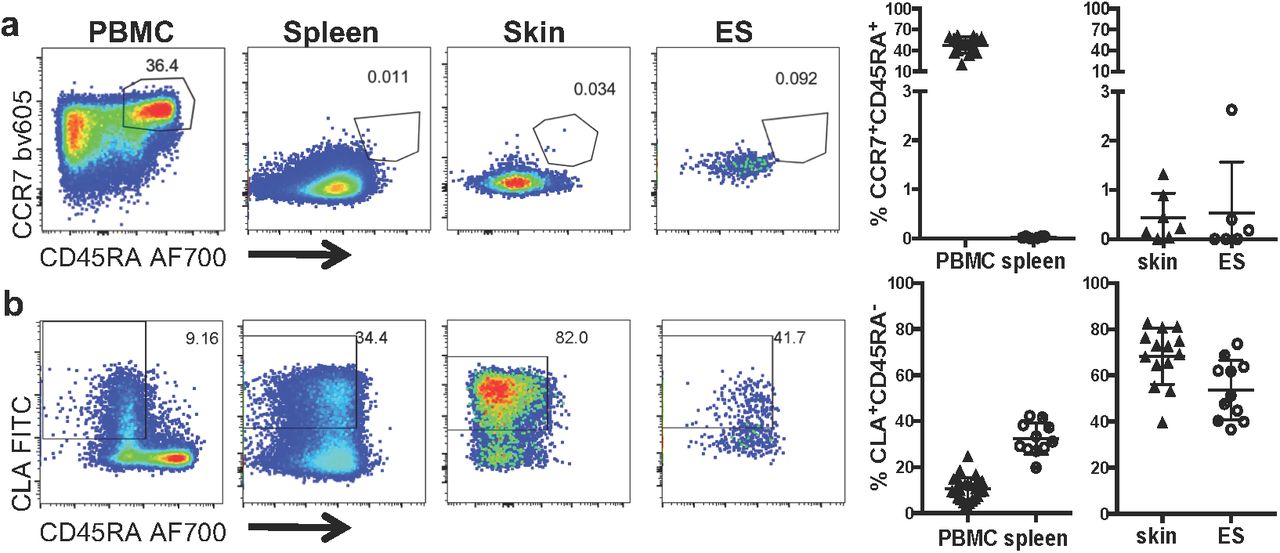
Representative flow cytometry analysis of (a) CCR7 and CD45RA expression, and (b) CLA and CD45RA expression by gated CD4+CD3+CD45+ live leukocytes from blood and skin of healthy donors, spleen and ES of huPBMC-ES-NSG mice and graphical summaryof the proportions of indicated cells by gated CD4+CD3+CD45+ live leukocytes. n=5- 6/experiment; cumulative data of 2 independent experiments.
Cutaneous CD4+ T cells are locally activated by microbial antigen
Skin CD4+ T cells play a crucial role in controlling cutaneous microbes (Belkaid and Tamoutounour 2016). Their specific role in responses against the commensal fungus Candida albicans (Lagunes and Rello 2016) is underlined by the fact that primary and acquired immunodeficiencies that lead to the impairment of CD4+ T cell immunity can cause pathogenic C.albicans infections (Gosselin et al. 2010; Klein et al. 1984; Lagunes and Rello 2016; Ling et al. 2015; Puel et al. 2011). Consistent with that, the human circulating T cell pool contains C.albicans-specific memory T cells (Acosta-Rodriguez et al. 2007; Hernández-Santos and Gaffen 2012).
We hypothesized that memory T cells specific for C.albicans, engraft in the ES and can mount a local antigen-specific T cell response upon encounter of microbial antigen. Therefore, we applied heat killed C.albicans (HKCA) to the ES in vivo. Injection of free HKCA failed to elicit a detectable expansion or proliferation in the spleen or ES of treated mice (Supp. Fig.1a-b; not shown). This was likely due to poor engraftment of HLA-DR+CD3- antigen presenting cells (APC) within the NSG strain (King et al. 2009) (Supp. Fig. 1c-d). Since C.albicans specific T cell responses depend on the presence of HLA-DR+ APC (Acosta-Rodriguez et al. 2007; Park et al. 2018) we pulsed autologous monocyte derived dendritic cells (moDC) with HKCA (HKCA/moDC) and injected these intradermally into the ES. LPS activated moDC (LPS/moDC) served as a control for non-specific activation of T cells by cytokines derived from activated APCs. Injections were repeated 3 times within 7 days and were followed by flow cytometry analysis of T cells isolated from the ES and spleen one week after the last injection (Fig. 5a). Whereas the proportion of human CD45+ cells in the spleen remained unaffected irrespective of the treatment, a slight increase in the percentage of human CD45+ cells could be detected in ES injected with HKCA/moDC compared to LPS/moDC injected ES (Fig. 5b). Additionally, an increased proportion of CD4+ T cells expressed the proliferation marker Ki67 and significantly upregulated CD25 upon injection of HKCA/moDC, indicating activation of CD4+ T cells in response to the encountered antigen (Fig. 5c). Interestingly the increased proliferation and activation of CD4+ T cells in response to antigen was locally restricted to the injected ES and absent in splenic T cells (Supp. Fig. 2a-b).

(a) Schematic outline of the experiment. (b) Graphical summary of the proportion of CD45+ cells among live cells in the lymphocyte gate in indicated organs of huPBMC-ES-NSG mice that received either LPS/moDC injections or HKCA/moDC injections into the ES. (c) Graphical analysis of the proportion of Ki67+ proliferating cells and CD25+ cells by gated CD4+CD3+CD45+ live leukocytes from LPS/moDC or HKCA/moDC treated ES. n=2-7/experiment, cumulative data of 2-5 independent experiments. Statistical significance determined by 2-tailed unpaired student’s t test; mean +/- SD. (d) Schematic: NSG mice bearing fully healed ES of one of two different skin donors (A and B) were adoptively transferred with either skin donor-matched PBMC or skin donor-mismatched PBMC. Intradermal injections of donor A derived LPS/moDC or HKCA/moDC were performed as depicted. Single cell suspensions of ES and spleen were analyzed by flow cytometry after ex vivo stimulation with PMA/Ionomycin and intracellular staining. (e-h) Graphical summary of the proportion of skin CD4+ T cells expressing the indicated markers following intradermal encounter of LPS/moDC (LPS) or HKCA/moDC (HKCA). Red data points represent CD4+ T cells isolated out of mismatched ES. Statistical significance determined by ANOVA and Tuckey’s test for multiple comparison; mean +/-SD. (i) Graphical summary of the ratio between CD4+ and CD8+ T cells of isolated skin T cells gated by CD3+CD45+ live leukocytes.
Together these data show that the huPBMC-ES-NSG model provides a tool to monitor antigen-specific T cell responses within human skin in vivo.
Antigen-specific T cell responses remain detectable in donor-mismatched skin tissue
So far, we used a completely matched system where ES, PBMC and moDC were from the same donor. However, access to skin that is matched to the PBMC, presents a limiting factor in studies of human immune responses. To broaden the model’s applicability, we sought to determine whether antigen-specific T cell responses could still be detected in the skin when using donor-mismatched tissues. Therefore, we compared cutaneous CD4+ T cell responses to HKCA in donor-matched and -mismatched ES. ES were generated from two different donors (donor A or B) designated ES-NSG-A and ES-NSG-B. After complete wound healing, both recipients received PBMC from donor A and were injected intradermally with matched LPS/moDC or HKCA/moDC (from donor A) (Fig. 5d).
Significantly higher proportions of CD4+ T cells from ES injected with HKCA/moDC expressed HLA-DR compared to LPS/moDC injected ES, indicating recent antigen-specific activation (Holling et al. 2004; Ko 1979; Oshima and Eckels 1990) (Fig. 5e). Moreover, ES injected with HKCA/moDC contained an increased proportion of CD4+ T cells secreting IL17 and TNFα compared to LPS/moDC (Fig. 5f-g). Importantly, IFNγ+ (Fig. 5h) and HLA-DR+ CD4+ cell proportions (Fig. 5e) were not expanded in allogeneic skin compared to the autologous setting. Additionally, CD4:CD8 ratios remained unchanged between skin T cells from matched and mismatched HKCA/moDC injected ES (Fig. 5i). Splenic CD4+ T cells showed high levels of activation irrespective of the injected moDC and no HKCA-specific cytokine production (Supp.Fig. 2c-f) and, splenic CD4+CD8+ T cell ratios were unaltered in response to the allogeneic ES (Supp. Fig. 2g), indicating the absence of a systemic response. Together, these data suggest that T cells were not activated by allogeneic keratinocytes or fibroblasts and that mismatched tissues still allow the study human antigen-specific cutaneous CD4+ T cell responses in the huPBMC-ES-NSG model.
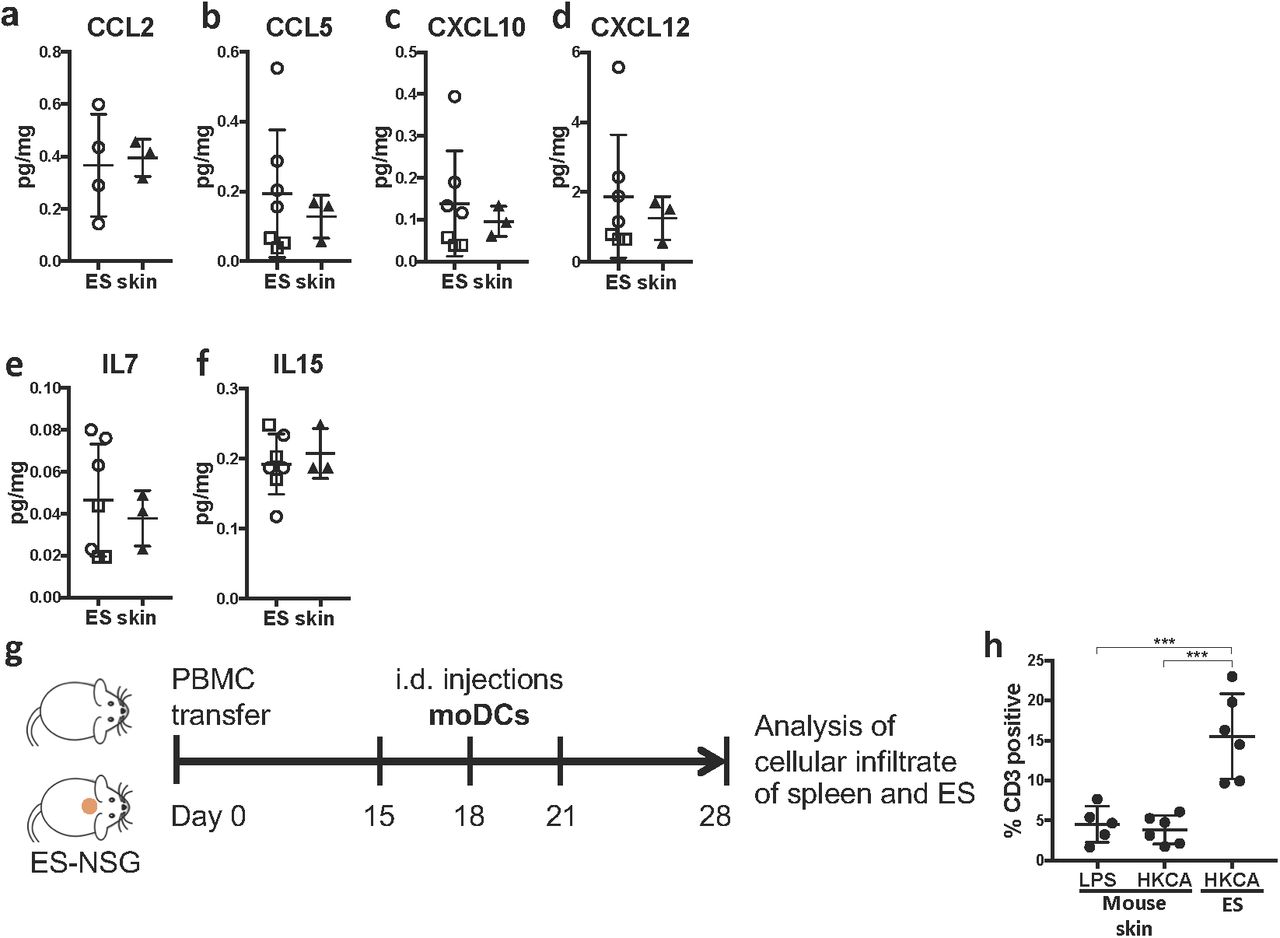
Human skin tissue promotes T cell maintenance and function
Based on the finding that human T cells preferentially infiltrated the human over the murine skin and T cells within the ES closely resembled T cells found in human skin (Fig. 1-3), we hypothesized, that human skin and ES provide similar signals to infiltrating T cells. Interestingly skin-derived chemokines, such as CCL2, CCL5, CXCL10 and CXCL12 (Fig. 6 a-d) and cytokines involved in T cell survival and maintenance, such as IL7 and IL15 were detectable at comparable levels in ES and normal human skin (Fig. 6 e,f). Based on these data, we hypothesized that the antigen-specific T cell response we detected was dependent on skin tissue-derived signals. To test this, we injected either the ES of huPBMC-ES-NSG or a defined area of murine skin on the back of huPBMC-NSG mice with autologous HKCA/moDC or LPS/moDC (Fig. 6g). Compared to ES treated with HKCA/moDC, significantly lower numbers of CD3+ cells infiltrated the murine skin. Importantly their frequency remained unaltered upon injection of HKCA/moDC, indicating a lack of antigen-specific activation (Fig. 6h). This suggests that the C.albicans specific T cell response detected in the huPBMC-ES-NSG model is not only a memory re-call response that is elicited by T cell-APC interaction, but requires tissue derived signals to support full memory T cell function.

Cytokine and chemokine expression within tissues was determined by bead-based multicomponent analysis of ES from huPBMC-ES-NSG and 3 different healthy human skin donors. (a-f) Amount of the indicated chemokines or cytokines per mg skin. (g) huPBMC-NSG mice received intradermal injections of LPS/moDC or HKCA/moDC into a defined patch of murine skin on the back of the mouse or into ES of huPBMC-ES-NSG mice. Single cell suspensions of injected murine skin regions were analyzed by flow cytometry 7 days after last i.d. injection as indicated. h) Graphical summary of the proportion of CD3+ T cells isolated from LPS/moDC (LPS) and HKCA/moDC (HKCA) injected murine skin and T cells isolated from the ES treated with HKCA/moDC (HKCA). Statistical significance determined by ANOVA and Tukey’s test for multiple comparison; mean +/-SD
Discussion
The majority of T cells in healthy human skin are CD45RO memory T cells that ensure adequate protective immunity on this peripheral barrier site (Bos et al. 1989; Klicznik et al. 2018; Watanabe et al. 2015). Most of our understanding of the development and function of protective T cell immunity in the skin is based on research using animal models with limited direct translation to humans (Di Meglio et al. 2011; Gudjonsson et al. 2007; Schreiner and King 2018). Therefore skin-humanized mouse models present a powerful platform to study cutaneous immune processes in vivo. Existing models in which PBMC and skin are grafted have been most useful for studying inflammatory processes of the skin (Boyman et al. 2004; Issa et al. 2010; Racki et al. 2010; Watanabe et al. 2015) but studies of human cutaneous immunity in steady-state in vivo have been difficult to realize. Additionally, healthy human skin contains a variety of adaptive and innate immune cells that impact the outcome of any intervention and study (Di Meglio et al. 2011; Klicznik et al. 2018; Pasparakis et al. 2014). Studying distinct immune processes in the skin requires simple traceable models, in which specific components can be independently manipulated. In that respect, neonatal foreskin grafts that contain 45-fold less T cells than adult human skin have been used to reduce the impact of resident cells (Watanabe et al. 2015), but even this tissue already contains T cells (Schuster et al. 2012). Here we combined engineered skin (ES) (Wang et al. 2000) devoid of any resident leukocytes, and adoptive transfer of human PBMC into immunodeficient NSG mice to generate a humanized mouse model (huPBMC-ES-NSG) that allows for specific study of individual immune cell populations, as well as the impact of tissue-derived signals on immunological processes in the skin.
Importantly, the use of ES permits precise control over the cell populations that partake in a specific immune response and targeted manipulation of keratinocytes and fibroblasts using CRISPR/Cas9 will facilitate to study the influence of selected pathways and the effects of these alterations on cutaneous immunity in vivo.
Poor engraftment of APC can limit antigen-specific T cell responses in vivo (King et al. 2009), which can be partly overcome by injection of DC loaded with antigen (Harui et al. 2011). However, we have found that antigen-specific recall responses require the support of the micromilieu, such as tissue-derived IL15 and IL7 (Belarif et al. 2018; Wang et al. 2011) and CD4+ T cells failed to respond to antigen presented in murine skin. Importantly, we found that healthy human skin-and ES-derived signals were remarkably similar, especially chemokines and cytokines involved in T cell recruitment and activation, such as CCL2 (Carr et al. 1994), CCL5 (Kawai et al. 1999), CXCL10 (Fukui et al. 2013), CXCL12 (Nanki and Lipsky 2001) and T cell function and maintenance, like IL7 (Adachi et al. 2015; Belarif et al. 2018) and IL15 (Adachi et al. 2015; Wang et al. 2011). This indicates that the huPBMC-NSG-ES model enables us to study the contribution of tissue-derived cues on cutaneous T cell maintenance and function.
Interestingly, the antigen-specific response was detectable in both, an autologous and an allogeneic setting. Thus, access to matched tissue samples is not limiting the study of cutaneous T cell responses in these humanized mice.
By engineering human skin tissue, we created an environment that allows the study of cutaneous T cell responses in absence of inflammation or infection in vivo. Additionally, the model may serve as a platform to test novel therapeutic interventions to treat cutaneous inflammation, tumors or autoimmune diseases. Taken together, the huPBMC-ES-NSG model provides a highly versatile tool to study cutaneous T cell responses and study and manipulate tissue-derived signals that impact skin immunity.
Material and Methods
Mice
Animal studies were approved by the Austrian Federal Ministry of Science, Research and Economy. NOD.Cg-Prkdcscid Il2rgtm1Wjl/SzJ (NSG) mice were obtained from The Jackson Laboratory and bred and maintained in a specific pathogen-free facility in accordance with the guidelines of the Central Animal Facility of the University of Salzburg.
Human specimens
Normal human skin was obtained from patients undergoing elective surgery, in which skin was discarded as a routine procedure. Blood and/or discarded healthy skin was donated upon written informed consent at the University Hospital Salzburg, Austria.
PBMC isolation for adoptive transfer into NSG recipients and flow cytometry
Human PBMC were isolated from full blood using Ficoll-Hypaque (GE-Healthcare; GE17- 1440-02) gradient separation. PBMC were frozen in FBS with 10% DMSO (Sigma-Aldrich; D2650), and before adoptive transfer thawed and rested overnight at 37°C and 5% CO2 in RPMIc (RPMI 1640 (Gibco; 31870074) with 5% human serum (Sigma-Aldrich; H5667 or H4522), 1% penicillin/streptomycin (Sigma-Aldrich; P0781), 1% L-Glutamine (Gibco; A2916801), 1% NEAA (Gibco; 11140035), 1% Sodium-Pyruvate (Sigma-Aldrich; S8636) and 0.1% β-Mercaptoethanol (Gibco; 31350-010). Cells were washed and 1.8-3×106 PBMC/mouse intravenously injected. Murine neutrophils were depleted with mLy6G (Gr-1) antibody (BioXcell; BE0075) intraperitoneally every 5-7 days as described before (Racki et al. 2010).
Generation of engineered skin (ES)
Human keratinocytes and fibroblasts were isolated from human skin and immortalized using human papilloma viral oncogenes E6/E7 HPV as previously described (Merkley et al. 2009). Cells were cultured in Epilife (Gibco, MEPICF500) or DMEM (Gibco; 11960-044) containing 2% L-Glutamine, 1% Pen/Strep, 10% FBS, respectively. Per mouse, 1-2×106 keratinocytes were mixed 1:1 with autologous fibroblasts in 400µl MEM (Gibco; 11380037) containing 1% FBS, 1% L-Glutamine and 1% NEAA for in vivo generation of engineered skin as described (Wang et al. 2000).
T cell isolation from skin tissues for flow cytometry
Healthy human skin and ES were digested as previously described (Sanchez Rodriguez et al. 2014). Approximately 1cm2 of skin was digested overnight in 5%CO2 at 37°C with 3ml of digestion mix containing 0.8mg/ml Collagenase Type 4 (Worthington; #LS004186) and 0.02mg/ml DNase (Sigma-Aldrich; DN25) in RPMIc. ES were digested in 1ml of digestion mix. Samples were filtered, washed and stained for flow cytometry or stimulated for intracellular cytokine staining. Approx. 3 cm2 of shaved dorsal mouse skin were harvested and single cell suspensions prepared as described (Gratz et al. 2014) and stained for flow cytometry.
Flow cytometry
Cells were stained in PBS for surface markers. For detection of intracellular cytokine production, spleen and skin single cell suspensions and PBMC were stimulated with 50 ng/ml PMA (Sigma-Aldrich; P8139) and 1 µg/ml Ionomycin (Sigma-Aldrich; I06434) with 10 µg/ml Brefeldin A (Sigma-Aldrich; B6542) for 3.5 hrs. For permeabilization and fixation Cytofix/Cytoperm (BectonDickinson; RUO 554714) or Foxp3 staining kit (Invitrogen; 00-5523-00) were used. Data were acquired on LSR Fortessa (BD Biosciences) or Cytoflex LS (Beckman.Coulter) flow cytometers and analyzed using FlowJo software (Tree Star, Inc.) A detailed list of the used antibodies can be found in the Supplements.
Histological staining of skin sections
Normal human skin, ES and adjacent murine skin were frozen in TissueTek (Sakura; TTEK). 7 µm cryosections were stained with Hemalum solution acid (Carl Rorth; T865.1) and Eosin Y aqueous solution (Sigma, 201192A). Human type VII collagen was stained by immunofluorescence using anti-human type VII collagen antibody and goat anti-rabbit A488 as secondary antibody, ProLongTM Gold Antifade Mountant with DAPI, (Invitrogen; P36931) was used for nuclear staining and mounting. For immunohistochemistry paraffin-embedded normal human skin and ES was stained for human Cytokeratin 5/6 according to the manufacturer’s protocol using a Ventana BenchMark Series automated slide stainer with ultraView Universal DAB Detection kit (Roche, 760-500).
Generation of monocyte derived dendritic cells (moDC)
moDC were generated from frozen PBMC similar to what has been described previously (Sallusto and Lanzavecchia 1994). Briefly, PBMC were thawed and monocytes adhered for 75 min at 37 °C and 5% CO2 in DC medium (RPMI 1640: 10% FBS, 2 mM L-Glutamine, 100 U/ml penicillin/streptomycin, 50 µM ß-mercaptoethanol). After washing, adherent monocytes were cultured in DC medium supplemented with 50 ng/ml GM-CSF (ImmunoTools; 11343127) and 50 ng/ml IL-4 (ImmunoTools; 11340047) for 7 days to generate immature DC. After 6 days, cells were harvested and re-plated in DC medium without cytokines. For activation, moDCs were cultured for 9-13 hrs with 5ng/ml LPS (Sigma-Aldrich; L2880) or 106 cells/ml heat killed Candida albicans (eubio; tlrl-hkca). 1.8-3×104 moDC/mouse were intradermally injected in 50µl PBS/mouse.
ProcartaPlexTM immunoassays from human skin and engineered skin
Human skin or ES from huPBMC-ES-NSG mice were stored at −70°C until use. Skin was taken up in PBS with Protease Inhibitor Cocktail (1:100) (Sigma-Aldrich; P8340) at 1ml/50mg skin, homogenized and filtered through 0.22µm SpinX columns. Suspensions were stored at −70°C until use. ProcartaPlex immunoassay was performed according to the manufacturer’s protocol and measured using Luminex Magpix(®) system.
Statistical analysis
Statistical significance was calculated with Prism 7.0 software (GraphPad) by one-way ANOVA with Tukey’s multiple comparisons test, or by un-paired student’s t-test as indicated. Error bars indicate mean +/- standard deviation.
Conflict of Interest
The authors declare no conflict of interest.
Author Contributions
IGK, EMM, MDR and MMK conceptualized the study, MMK, EMM and IGK designed the experiments; MMK, AB, LMG and RH acquired the data; ML performed IHC staining, AS, RR, and A.Sir acquired human samples; MMK performed data analysis, MMK and IGK interpreted the data and wrote the manuscript. All authors reviewed the final version of the manuscript. IKG and EMM supervised the project.
Supplemantary Figures

(a) Experimental procedure of the injection of 5×104 free HKCA cells into the ES. Single cell suspensions of indicated organs were analyzed by flow cytometry. (b) Graphical summary of human CD45+ cell proportions of live leukocytes in spleen and ES of mice that were left untreated (untrtd), injected with PBS or HKCA. (c) Representative flow cytometry analysis of CD3-HLA-DR+ cells in human PBMC, skin and spleen and ES of huPBMC-ES-NSG and (d) graphical summary gated on live CD45+ cells.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
(a-f) Graphical summary of the expression of indicated markers by CD4+ T cells of CD3+CD45+ live leukocytes isolated from the spleen of huPBMC-ES-NSG mice after intradermal injection of LPS/moDC (LPS) or HKCA/moDC (HKCA) upon ex vivo stimulation with PMA/ionomycin and intracellular cytokine staining. (g) Ratio of CD4+ to CD8+ cells in spleens of huPBMC-ES-NSG mice, gated on CD3+CD45+ live leukocytes.
Detailed list of antibodies and reagents
Acknowledgements
We especially thank all human subjects for blood and skin donation and the nurses at the Breast Center University Hospital of the Paracelsus Medical University Salzburg, Austria. We thank Dr. Stefan Hainzl, EB House Austria, Department of Dermatology, University Hospital of the Paracelsus Medical University Salzburg, Austria, for the immortalization of primary human keratinocytes and fibroblasts. We thank Monika Prinz from the Department of Dermatology at the University Hospital of the Paracelsus Medical University Salzburg, Austria for help with the IHC staining and Peter Steinbacher from the Department of Biosciences at the University of Salzburg, Austria, for support with microscopy. This work was supported by the Focus Program “ACBN” of the University of Salzburg, Austria, by a grant from the Dystrophic Epidermolysis Bullosa Research Association (DEBRA) International and DEBRA Austria, and NIH grant R01AI127726. MMK is part of the PhD program Immunity in Cancer and Allergy, funded by the Austrian Science Fund (FWF, grant W 1213) and was recipient of a DOC Fellowship of the Austrian Academy of Sciences.
References




