

Abstract
Background Mycoplasma genitalium is a common cause of non-gonococcal non-chlamydial urethritis and cervicitis. Testing of asymptomatic populations has been proposed, but prevalence rates in asymptomatic populations are not well established. We aimed to estimate the prevalence of M. genitalium in adults in the general population, in clinic-based samples, pregnant women, men who have sex with men (MSM) and female sex workers (FSW).
Methods We searched Embase, Medline, IndMED, AIM and LILACS from 1 January 1991 to 12 July 2016 without language restrictions. We included studies with 500 participants or more. We screened and selected studies and extracted data in duplicate. We examined eligible studies in forest plots and conducted random effects meta-analysis to estimate prevalence, if appropriate. Between study heterogeneity was examined using the I2 statistic and meta-regression.
Results Of 3,316 screened records, 63 were included. In randomly selected samples from the general population, the summary prevalence estimate was 1.3% (95% confidence intervals, CI 1.0 to 1.8%, I2 41.5%, 3 studies) in countries with higher levels of development and 3.9% (95% CI 2.2 to 6.7, I2 89.2%, 3 studies) in countries with lower levels. Prevalence estimates were similar in women and men (p=0.47). In clinic-based samples prevalence estimates were higher, except in asymptomatic patients (0.8%, 95% CI 0.4 to 1.4, I2 0.0%, 3 studies). Summary prevalence estimates were: pregnant women 0.9% (95% CI 0.6 to 1.4%, I2 0%, 4 studies); MSM in the community 3.2% (95% CI 2.1 to 5.1, I2 78.3%, 5 studies); FSW in the community 15.9% (95% CI 13.5 to 18.9, I2 =79.9%, 4 studies).
Discussion This systematic review can inform testing guidelines for M. genitalium infection. The low estimated prevalence of M. genitalium in the general population, pregnant women and asymptomatic attenders at clinics does not support expansion of testing to asymptomatic people in these groups.
Registration Numbers
PROSPERO: CRD42015020420
Introduction
Mycoplasma genitalium is a cause of non-gonococcal non-chlamydial urethritis in men and cervicitis in women,1-3 and is reported to be associated with pelvic inflammatory disease, infertility and preterm birth.4 M. genitalium was first isolated in the early 1980s in men with non-gonococcal urethritis (NGU)5 but, owing to difficulties in detecting the microorganism by culture, most research on M. genitalium has been done since the development of nucleic acid amplification tests (NAAT) in the early 1990s.1 In populations studied in healthcare settings, M. genitalium has been detected in substantial proportions of study participants.1 2 Based on these studies, routine testing has been suggested to detect and treat M. genitalium in asymptomatic attenders in healthcare settings6 and the recommendation has also been extended to low-risk general populations.7 Multiplex NAAT are being used increasingly to detect multiple sexually transmitted pathogens,8 9 increasing pressure for their routine use.
Criteria for assessing the appropriateness of screening for a disease in the population include requirements that the disease is an important public health problem and that screening has been shown to do more good than harm.10 The prevalence of M. genitalium in asymptomatic populations has not been ascertained systematically. Non-systematic reviews have reported prevalence estimates ranging from zero to 0.7% to 3.3% in the general population1 and from zero to 20% in a range of female study populations described as ‘low-risk’.11 The objectives of this study were to systematically review the literature about the prevalence of M. genitalium in the general population and in specific groups (men who have sex with men, MSM, female sex workers, FSW, pregnant women, consecutively enrolled attenders in clinics).
Methods
We followed a predefined review protocol.12 This report presents the findings of the first of three review questions (prevalence of M. genitalium). Two other review questions (incidence and persistence of untreated M. genitalium infection) will be addressed in a separate report. We report the findings using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA, checklist in online Appendix, text S1).13
Eligibility Criteria
We included studies that provided an estimate of the prevalence of M. genitalium infection in urogenital or rectal samples from women and men older than 13 years in any country from 1991 onwards, when the first NAAT was described.1 We included studies conducted amongst people in the general population or amongst attenders at healthcare settings. Eligible study designs were cross-sectional studies, cohort studies and baseline data in randomised controlled trials, published as full papers, abstracts or conference posters. We excluded laboratory studies, studies restricted to people with a specific condition, e.g., men with urethritis, women with abnormal cervical smears and women with pregnancy complications. To reduce small study effects, we restricted the review to larger studies that tend to use more rigorous study methodology and are at lower risk of bias.14 After screening titles and abstracts, we determined that inclusion of studies with 500 participants or more would result in at least 20 studies in the review.
Information sources and search strategy
We searched Medline, Embase, African Index Medicus, IndMED, and LILACS databases from 1st January 1991 to 12th July 2016 without language restrictions. The full search strategy for Medline and Embase is provided in the online Appendix (Text S2). The other databases were searched using only the term “Mycoplasma genitalium.” We used Endnote (version 7, Thomson Reuters) to import, de-duplicate and manage retrieved records.
Study selection
Two reviewers independently screened the identified records using pre-piloted checklists to assess eligibility, first of abstracts and titles and then of full text records. Differences were resolved by discussion or adjudication by a third reviewer. When multiple records reported on the same study population, we defined a primary record to represent the study, based on a combination of the following factors: description as a main paper by the authors, most detailed report of methods, prevalence reported as the main result and date of publication.
Data collection process and data items
Two researchers extracted data independently for every included study, using a piloted extraction form in an online database (Research Electronic Data Capture, REDCap, Vanderbilt University, Tennessee). We resolved differences by discussion. The data extraction form included items about: study design, demographic characteristics, sample size, methods of participant selection and specimen collection, response rates, number of infected participants and number tested and reported prevalence estimates (with 95% confidence intervals, CI) overall and for prespecified subgroups.
We also recorded a measure of the level of development of the country in which the study was done using the human development index (HDI) 2015 HDI-dataset,15 which we categorised as higher (combining very high and high) or lower (medium and low). We defined studies a priori as ‘general population’ if they used any method to draw a random sample from the population of a whole country or a region, or as ‘community based’ if participants were enrolled outside healthcare settings but used non-random methods such as convenience sampling, snowball, or respondent driven sampling. Studies conducted in healthcare settings were coded according to their study population: clinic attenders, pregnant women, MSM and FSW. Studies that had enrolled participants from both healthcare settings and the community and did not stratify results were coded as clinic-based studies. We labelled studies according to the country in which the fieldwork was done and assigned numbers after the country name if there was more than one study from the same country. We generated separate strata within studies if they included participants from more than one country or from more than one relevant population subgroup, e.g. MSM and heterosexual adults.
Risk of bias in individual studies
To evaluate the individual studies, we adapted an instrument from another systematic review of studies of Chlamydia trachomatis prevalence (online Appendix, text S3).16 Two reviewers independently assessed each item as being at high, low or uncertain risk of bias. Differences were resolved by discussion.
Summary measure and synthesis of results
The outcome was the estimated prevalence (and 95% CI), defined as the number of specimens with a positive M. genitalium test result divided by the number of eligible participants with a valid test result. Where possible, we confirmed the published values using raw numbers reported in the publication. In studies that reported weighted prevalence estimates and confidence intervals or where raw numbers were not available, we used the information reported by the authors. We calculated survey response rates, whenever possible, by dividing the number of participants tested by the number of eligible people asked to participate.
We initially examined the estimates of M. genitalium prevalence visually in forest plots. We stratified studies, based on a previous study showing factors that contribute to heterogeneity in estimates of C. trachomatis prevalence,16 by: sampling method (random sample of the general population, community-based, or clinic-based); study population (general population, pregnant women, MSM, FSW); HDI (higher or lower); and, where reported, by sex and age of participants as under 25 years or 25 years and older.
We used the I2 statistic to assess heterogeneity that was not due to random variation.17 Heterogeneity was considered moderate or high when I2 was greater than 50% or 75% respectively. We used random effects meta-analysis to combine prevalence estimates where appropriate, assuming that, even when results were stratified, there might be real differences in M. genitalium prevalence between studies. We log-transformed the prevalence estimates and 95% CI before meta-analysis and back-transformed the summary average prevalence (and 95% CI) to the natural scale. We did not conduct meta-analysis on the logit scale because the log odds and confidence intervals could not be obtained from studies that reported weighted prevalence estimates. We calculated a prediction interval to provide information about the likely range of prevalence in future studies done in similar study populations if more than three studies contributed to a subgroup and if between-study heterogeneity was low (I2<50%).18 We did a meta-regression analysis to examine possible factors (HDI, use of probability sampling, sample size, response rate, sex and use of adequate sample and target populations) contributing to heterogeneity in general population and clinic-based studies. Analyses were done using the ‘metan’ and ‘metareg’ commands in Stata (Stata 13, Stata Corp, Austin, Texas, USA).
Results
Search results
We screened the titles and abstracts of 3,316 unique records published after 1991 and the full text of 833 studies (Figure S1 in online Appendix). A total of 63 records was included with participants who were; sampled at random from the general population19-24 or using alternative community-based methods,25-29 MSM and male-to-female transgendered,30-35 FSW,36-40 and pregnant women.41-44 Of these, 37 studies included patients attending healthcare settings.8 45-80 We report results using the country name and number of the study or subgroup within a study.
Table 1 shows that most characteristics of included studies were similar to those of studies excluded because the sample size was below 500 (details in Table S1, online Appendix). The distribution of included and excluded studies was broadly similar. Eight of the excluded studies included participants from the community, but all studies that used probability-based sampling methods were included.
Characteristics of included and excluded studies
Risk of bias in individual studies
No study was at low risk of bias in all domains (Figure S2). The studies at lowest risk of bias were those that used probability sampling in the general population. Only one study compared responders and non-responders and that study found differences between these groups.24 Reporting of complete results, including CIs and baseline data, was considered adequate in 22 studies.
Studies in the general population and community
We included 11 studies, six of which were in countries with higher HDI (Denmark 1,23 Great Britain 2 and Great Britain 4,24 25 Norway 4,26 Russian Federation 327 and USA 2,19 N=13,331) and five in countries with a lower (Honduras 1,20 Vietnam 1,21 Kenya 1,28 Madagascar 1,29 Tanzania 1,22 N=4,978) HDI (Figure 1, Table S2 in online Appendix).
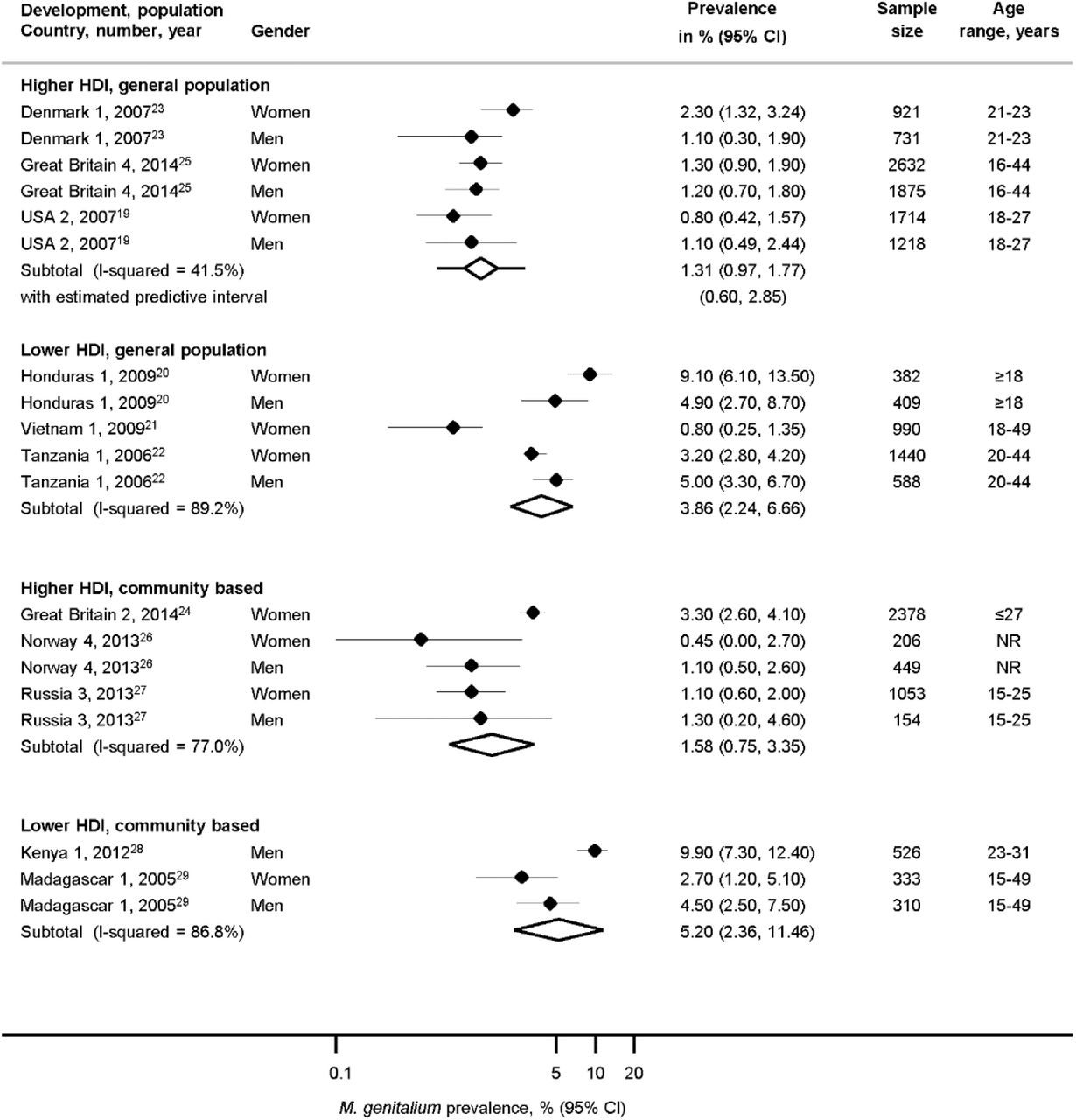
Estimated prevalence of Mycoplasma genitalium in randomly selected samples of the general population or in other community-based samples, by human development index.
CI, confidence interval; HDI, human development index. Solid diamond and lines show the point estimate and 95% confidence intervals for each study. The diamond shows the point estimate and 95% confidence intervals of the summary estimate. Lines extending from the diamond show the prediction interval. The prevalence estimates are plotted on a logarithmic scale.
The summary average general population prevalence of M. genitalium in three studies in countries with higher HDI was 1.3% (95% CI 1.0 to 1.8%, prediction interval 0.6, 2.9%, I2 41.5%, N=9,091, Figure 1), with low between-study heterogeneity in three studies (one region in Denmark 1,23 or the whole population in Great Britain 4 and USA 2).19 24 In three studies in higher HDI countries that enrolled participants using convenience sampling methods from sub-national communities (N=4,240, Table S2), between-study heterogeneity was higher than in the studies that used random sampling methods but the summary average prevalence was similar (1.6%, 95% 0.8 to 3.4%, I2 77.0%).25-27 Amongst adults under 25 years, average M. genitalium prevalence was 1.7% (95% CI 1.0 to 2.6%, I2 80.3%) in women and 0.3% in men (0.1 to 1.4%, I2 91.3%) (Figure S3 in online Appendix). There were too few estimates from adults aged 25 years and over to compare estimates between women and men.
The surveys from five countries with lower HDI enrolled very different populations M. genitalium prevalence estimates were more variable (Figure 1, Table S2 in online Appendix).20-22 28 29 The summary estimate of prevalence in three studies that used probability sampling was 3.9% (2.2 to 6.7, I2 89.2%) and, in two studies that used other methods to enrol participants from community settings, 5.2% (2.4 to 11.5, I2 86.8%).
In a meta-regression analysis that compared characteristics of all studies in adults in the general population, there was some statistical evidence to suggest higher estimates of M. genitalium prevalence in countries with lower than higher HDI (difference 3.1%, 95% CI −0.1 to 6.3%, p=0.057) but no statistical evidence of a difference by sex (0.9%, 95% CI −1.6 to 3.3% p=0.47) or for other study related variables that were examined (Table S3 in online appendix).
Pregnant women in antenatal clinics and women in the general population
We included four studies in pregnant women before 14 weeks gestation, all in countries with higher HDI (N=3,472, age range 16 to 48 years; France 2,44 Great Britain 1,41 Japan 1,42 and USA 5,43 Figure 2, Table S4 in online Appendix). The combined average prevalence was 0.9% (95% CI 0.6 to 1.4%, prediction interval 0.4, 2.3%, I2 0%). The estimated prevalence was slightly lower than in the three studies in women in the general population (1.4%, 95% CI 0.8 to 2.4%, I2 73.4%) but confidence intervals overlapped.
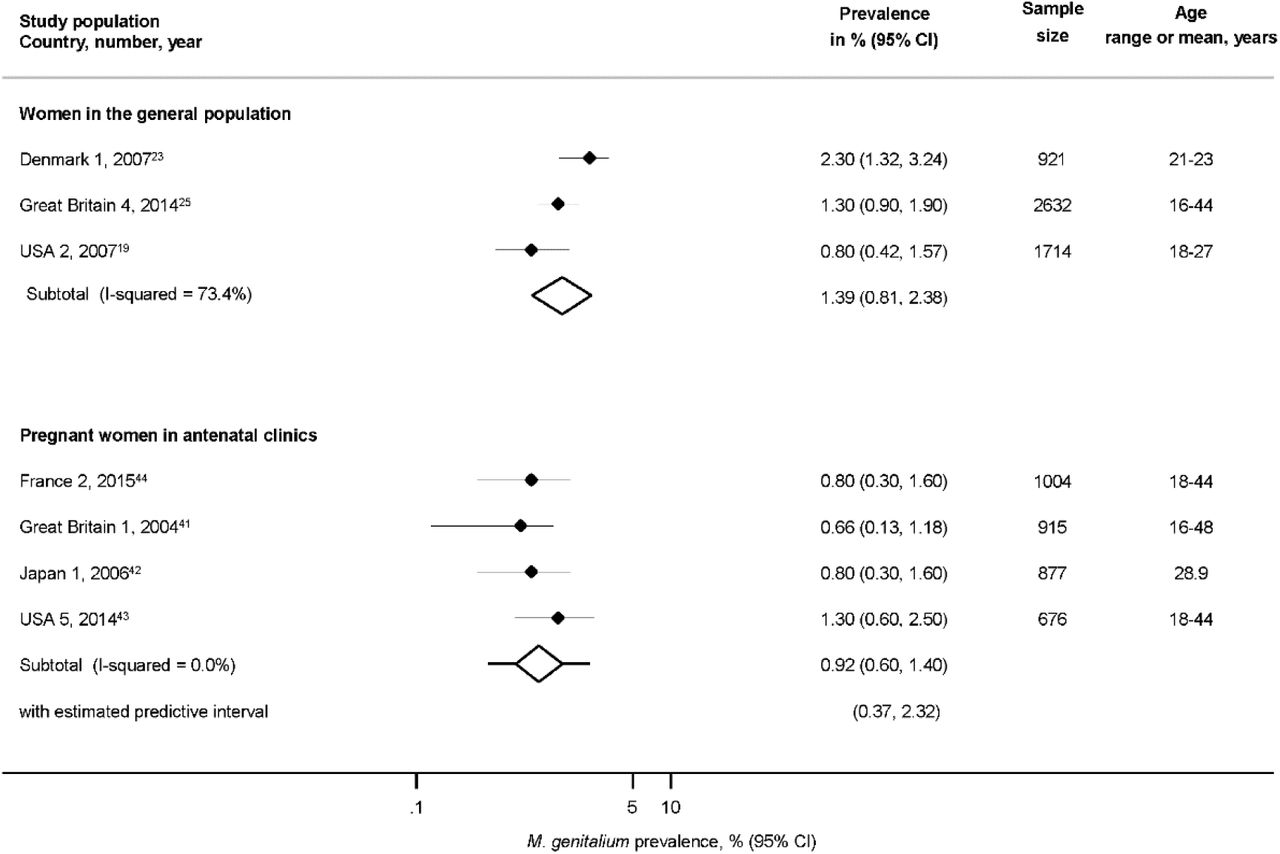
Estimated prevalence of Mycoplasma genitalium in pregnant women in antenatal clinics and in randomly selected samples of women in the general population.
CI, confidence interval. Solid diamond and lines show the point estimate and 95% confidence intervals for each study. The diamond shows the point estimate and 95% confidence intervals of the summary estimate. Lines extending from the diamond show the prediction interval. The prevalence estimates are plotted on a logarithmic scale.
MSM and FSW in community-based and clinic-based studies
Five studies from four records enrolled MSM from the community (Figure 3, Table S4 in online Appendix) in specific areas in; Australia 2,30 El Salvador 1,31 Guatemala 1 and Honduras 3,32 and Nicaragua 1,33 (N=3,012). The summary average prevalence in these studies was 3.2% (95% CI 2.1 to 5.1%, I2 78.3%) with moderate between-study heterogeneity. The summary average estimate of M. genitalium prevalence in MSM enrolled from clinics in Germany 3,55 the Netherlands 2,54 Norway 535 and USA 334 was 3.7% (95% CI 2.4 to 5.6%, I2 78.5%).

{kind=link}
{kind=link}
{kind=link}
Estimated prevalence of Mycoplasma genitalium in community-based and clinic-based samples of men who have sex with men and female sex workers
CI, confidence interval; FSW, female sex workers; MSM, men who have sex with men; NR, not reported. Solid diamond and lines show the point estimate and 95% confidence intervals for each study. The diamond shows the point estimate and 95% confidence intervals of the summary estimate. Lines extending from the diamond show the prediction interval. The prevalence estimates are plotted on a logarithmic scale.
Studies that enrolled FSW were more variable. Estimated M. genitalium prevalence in the community-based studies in specific areas in southwest China 2,36 northern Germany 1,37 Honduras 2,38 and Uganda 139 was 15.9% (95% CI 13.5 to 18.9%, N=4,006, I2 79.9%). In one study that enrolled FSW from a clinic in Benin and Ghana 1,40 the estimated prevalence was higher (26.3%, 95% CI 23.3 to 29.4%).40
Clinic-based studies, unselected populations
We included 37 studies from 14 countries, of which 24 were from Australia, Great Britain, Norway, South Korea and Sweden (Table S5, Figure S4 in online Appendix). Estimates of M. genitalium were very heterogeneous (I2 >95%), except for studies that only included patients without symptoms,8 50 64 (N=2889, 0.8%, 95% CI 0.4 to 1.4%, I2 0%). Most study populations included patients both with and without symptoms. The lowest estimate was reported in a fertility clinic population in Venezuela 178 (N=3,358, 0.6%, 95% CI 0.3 to 0.9%). The highest estimates were from patients attending youth clinics in Russia 1(N=9,208, 12.6%, 95% CI 11.9 to 13.3%), women attending primary health care clinics in Limpopo province, South Africa 163 (N=601, 8.7%, 95% CI 6.4 to 10.9%) and STI clinic attenders in Sweden 873 (N=679, 7.4% 95% CI 5.5 to 9.6%) and the USA 477 (N=1,090, 7.7%, 95% CI 6.2 to 9.4%).
Discussion
Main Findings
In large nationally representative surveys conducted in very highly developed countries the summary average prevalence estimate of M. genitalium was 1.3% (95% CI 1.0 to 1.8%,3 studies, I2 41.5%) in adults aged 16 to 44 years with no statistical evidence of a difference between men and women (p=0.47). Summary prevalence estimates in specific subpopulations were: pregnant women 0.9% (0.6 to 1.4%), MSM in community samples 3.2% (2.1 to 5.1%, 5 studies, I2 78.3%) and MSM in clinic-based samples 3.7% (2.4 to 5.6%, 4 studies, I2 78.5%). Prevalence estimates were higher in FSW, ranging from 13.2% in one community-based study to 26.3% in one clinic-based study. In clinic-based surveys, prevalence estimates varied from 0.8% (95% CI 0.4 to 1.4%, 3 studies, I2 0%) in patients with no symptoms to 12.6% (95% CI 11.9 to 13.3%) in one study in Russia.
Strengths and limitations
The broad search strategy is a strength of this review. It allowed for identification of a wide range of different studies and it is unlikely that we missed large studies. The a priori defined inclusion criteria allowed a clear selection process for the detected studies and duplicate screening and data extraction prevented data entry errors. By including only studies with 500 participants or more, we aimed to reduce the influence of small study biases that can distort results. This strategy included all studies that used methods to select random samples of the general population and provided summary estimates with little heterogeneity for general population samples in very highly developed countries, pregnant women and asymptomatic people attending outpatient healthcare settings. Although we explored between-study heterogeneity using meta-regression analysis, we did not identify factors that could explain a substantial proportion of the heterogeneity. A further limitation to interpretation is that we could not provide prediction intervals for most subgroups because the method used to estimate prediction intervals is not suited to situations with few studies or where heterogeneity or the risk of bias are high.18 Finally, we could not assess an earlier finding, in surveys of chlamydia prevalence,16 that lower response rates are associated with higher prevalence estimate because very few studies reported these results. Amongst studies that reported response rates we did not find an association with M. genitalium prevalence (Table S3 in online Appendix).
Interpretation and comparison with other studies
To our knowledge, this is the first systematic review assessing the prevalence of M. genitalium in different population groups including those outside healthcare settings. Our findings suggest that M. genitalium might be less prevalent than C. trachomatis in the general population but comparison is not straightforward. In a systematic review of population-based surveys of C. trachomatis, estimated prevalence in adults <27 years in high-income countries was 4.3% (95% CI 3.6 to 5.0%, I2 0%) in women and 3.6% (95% CI 2.8 to 4.4%, I2 6.2%) in men,16 compared with our summary estimates of less than 2% for M. genitalium in women and men <25 years old. Within studies that tested for both pathogens, prevalence estimates for M. genitalium and C. trachomatis were similar in Great Britain,24 but higher for C. trachomatis than M. genitalium in Denmark23 and the USA.19 It is, however, possible that M. genitalium prevalence has been underestimated because the sensitivity of NAATs is lower than previously believed.9 In general, age differences seem less marked amongst women for M. genitalium than for C. trachomatis, where prevalence after age 25 years is much lower than in younger women. Age-specific patterns of M. genitalium were, however, difficult to discern with certainty, largely because population-based studies that provided age-stratified estimates used non-comparable age groups and only two had estimates for participants older than 25 years (Norway 4 and Great Britain 4 studies).
In clinic-based surveys, participant selection methods and characteristics differed substantially between different types of clinics and countries. M. genitalium prevalence estimates were consistent and comparable (or even lower) than in general population-based surveys in studies that only enrolled asymptomatic patients or pregnant women in antenatal clinics. Amongst MSM, estimated M. genitalium prevalence was similar in community-based and clinic-based studies.
Implications for clinical practice, policy and research
This systematic review provides evidence about the prevalence of M. genitalium that can be used in mathematical modelling studies and to inform testing guidelines for infection. The trend for molecular diagnostic tests to include targets that identify multiple sexually transmitted pathogens means that testing for asymptomatic M. genitalium infection will become more widespread. In clinical settings, systematic reviews of the prevalence of M. genitalium in symptomatic non-gonococcal non-chlamydial urethritis and of resistance to macrolides and fluoroquinolones would further help to refine clinical treatment guidelines for M. genitalium infections. The absence of randomised controlled trials that demonstrate a clinical benefit of screening and the increasing prevalence of resistance to azithromycin are reasons for restricting widespread testing for M. genitalium.81 The low estimated prevalence of M. genitalium in the general population, in pregnant women and in asymptomatic attenders in health care settings and absence of a clearly defined age group at higher risk of infection do not provide strong support for the appropriateness of universal or age-based screening programmes for M. genitalium in these population groups.
Key messages
Routine screening for Mycoplasma genitalium infection has been proposed, but prevalence rates are not well established
In samples from the general population, the summary prevalence estimate is 1.3% in countries with higher development and 3.9% in countries with lower development
M. genitalium prevalence in the general population and differences in prevalence by age appear to be less than for Chlamydia trachomatis
The low prevalence estimates in the general population, pregnant women and asymptomatic clinic-based patients do not support universal screening for M. genitalium
Funding
This study received funding from the Swiss National Science Foundation (grant numbers 320030_173044 and 320030_135654)
Competing interests
Nicola Low is deputy editor of Sexually Transmitted Infections. All other authors declare no conflicts of interest.
Author contributions
Conceived and designed the review; NL, LB, MC, PS, DE. Screened titles, abstracts and full text; LB, MC, DE, HA, GL, NL. Extracted data; LB, MC, DE, HA, G-RL. Analysed data; LB, MC, FH, MG. Wrote the first draft; LB, MC. Revised the paper; NL, MG, FH, DE, PS, HA. Approved the final version; LB, MC, DE, MG, FH, PS, HA, NL.
Author contributions
We would like to thank Georgia Salanti for her advice about meta-analysis.
References




